-
0
Patient Assessment
- 0.1 Patient demand
- 0.2 Overarching considerations
- 0.3 Local history
- 0.4 Anatomical location
- 0.5 General patient history
-
0.6
Risk assessment & special high risk categories
- 5.1 Risk assessment & special high risk categories
- 5.2 age
- 5.3 Compliance
- 5.4 Smoking
- 5.5 Drug abuse
- 5.6 Recreational drugs and alcohol abuse
- 5.7 Parafunctions
- 5.8 Diabetes
- 5.9 Osteoporosis
- 5.10 Coagulation disorders and anticoagulant therapy
- 5.11 Steroids
- 5.12 Bisphosphonates
- 5.13 BRONJ / ARONJ
- 5.14 Radiotherapy
- 5.15 Risk factors
-
1
Diagnostics
-
1.1
Clinical Assessment
- 0.1 Lip line
- 0.2 Mouth opening
- 0.3 Vertical dimension
- 0.4 Maxillo-mandibular relationship
- 0.5 TMD
- 0.6 Existing prosthesis
- 0.7 Muco-gingival junction
- 0.8 Hyposalivation and Xerostomia
- 1.2 Clinical findings
-
1.3
Clinical diagnostic assessments
- 2.1 Microbiology
- 2.2 Salivary output
-
1.4
Diagnostic imaging
- 3.1 Imaging overview
- 3.2 Intraoral radiographs
- 3.3 Panoramic
- 3.4 CBCT
- 3.5 CT
- 1.5 Diagnostic prosthodontic guides
-
1.1
Clinical Assessment
-
2
Treatment Options
- 2.1 Mucosally-supported
-
2.2
Implant-retained/supported, general
- 1.1 Prosthodontic options overview
- 1.2 Number of implants maxilla and mandible
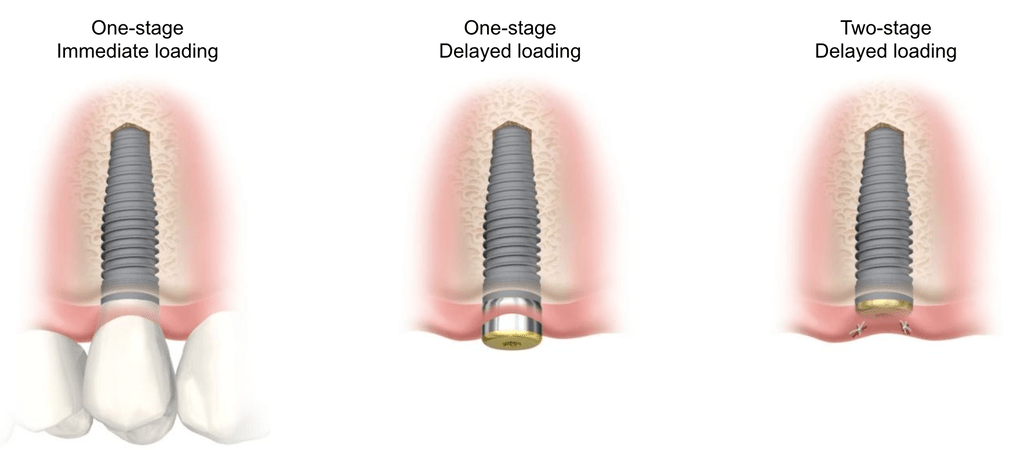
- 1.3 Time to function
- 1.4 Submerged or non-submerged
- 1.5 Soft tissue management
- 1.6 Hard tissue management, mandible
- 1.7 Hard tissue management, maxilla
- 1.8 Need for grafting
- 1.9 Healed vs fresh extraction socket
- 1.10 Digital treatment planning protocols
- 2.3 Implant prosthetics - removable
-
2.4
Implant prosthetics - fixed
- 2.5 Comprehensive treatment concepts
-
3
Treatment Procedures
-
3.1
Surgical
-
3.2
Removable prosthetics
-
3.3
Fixed prosthetics
-
3.1
Surgical
- 4 Aftercare
Time to function
Key points
- Main considerations of 'time to function' are immediate, early and conventional time frames for restored function
- When specific criteria and protocols are met, immediate function is regarded as providing a safe and predictable treatment outcome
- Immediate function may logically reduce overall treatment time and eliminate the need for the edentulous patient to wear a temporary removable prosthesis

Conventional Function
Traditional endosseous oral implant treatment protocols ad modum Brånemark required a variable healing period (usually 3-6 months) before prosthesis placement. The healing period was considered necessary to achieve osseointegration and establish a load-bearing interface. The traditional protocol is referred to as “conventional function” and has yielded very good long-term clinical results.
Early function
“Early function” refers to prosthesis placement from 3 days to 3 months after implant placement. Compared to immediate and conventional function protocols, it has lead to comparable documented clinical outcomes.
Immediate function
The prosthesis loading protocol change to one occuring within 3 days of implant placement is referred to as “immediate function”. It has led to promising documented clinical outcomes when judged in the context differences in bone loss, prosthesis- or implant failure, when compared to “delayed function” documentation. Advantages for the patient include reduction in time from implant placement to restored function, an overall reduction in treatment time and elimination of the need to wear a temporary removable prosthesis.
Current experience indicates that oral implants with good primary stability are candidates for immediate function. Primary stability is popularly ascertained either through the surgeon’s feel or through a surrogate measure of stability (insertion torque or resonance frequency analysis RFA). In the absence of good primary implant stability an immediate function protocol is contraindicated.
While immediate function can be considered in many treatment scenarios, the probability of success increases if multiple implants are placed and the immediate function prosthesis “splints” implants together. This augurs well for the use of immediate function protocols for the edentulous maxilla and mandible where multiple implants are routinely placed to support both a provisional and definitive fixed prosthesis.