-
0
Patient Assessment
- 0.1 Patient demand
- 0.2 Overarching considerations
- 0.3 Local history
- 0.4 Anatomical location
- 0.5 General patient history
-
0.6
Risk assessment & special high risk categories
- 5.1 Risk assessment & special high risk categories
- 5.2 age
- 5.3 Compliance
- 5.4 Smoking
- 5.5 Drug abuse
- 5.6 Recreational drugs and alcohol abuse
- 5.7 Parafunctions
- 5.8 Diabetes
- 5.9 Osteoporosis
- 5.10 Coagulation disorders and anticoagulant therapy
- 5.11 Steroids
- 5.12 Bisphosphonates
- 5.13 BRONJ / ARONJ
- 5.14 Radiotherapy
- 5.15 Risk factors
-
1
Diagnostics
-
1.1
Clinical Assessment
- 0.1 Lip line
- 0.2 Mouth opening
- 0.3 Vertical dimension
- 0.4 Maxillo-mandibular relationship
- 0.5 TMD
- 0.6 Existing prosthesis
- 0.7 Muco-gingival junction
- 0.8 Hyposalivation and Xerostomia
- 1.2 Clinical findings
-
1.3
Clinical diagnostic assessments
- 2.1 Microbiology
- 2.2 Salivary output
-
1.4
Diagnostic imaging
- 3.1 Imaging overview
- 3.2 Intraoral radiographs
- 3.3 Panoramic
- 3.4 CBCT
- 3.5 CT
- 1.5 Diagnostic prosthodontic guides
-
1.1
Clinical Assessment
-
2
Treatment Options
- 2.1 Mucosally-supported
-
2.2
Implant-retained/supported, general
- 1.1 Prosthodontic options overview
- 1.2 Number of implants maxilla and mandible
- 1.3 Time to function
- 1.4 Submerged or non-submerged
- 1.5 Soft tissue management
- 1.6 Hard tissue management, mandible
- 1.7 Hard tissue management, maxilla
- 1.8 Need for grafting
- 1.9 Healed vs fresh extraction socket
- 1.10 Digital treatment planning protocols
- 2.3 Implant prosthetics - removable
-
2.4
Implant prosthetics - fixed
- 2.5 Comprehensive treatment concepts
-
3
Treatment Procedures
-
3.1
Surgical
-
3.2
Removable prosthetics
-
3.3
Fixed prosthetics
-
3.1
Surgical
- 4 Aftercare
Healed vs fresh extraction socket
Key points
- Short term survival of implants placed in healed vs. fresh extraction sockets seems similar
- Long-term data on this subject are limited
Introduction
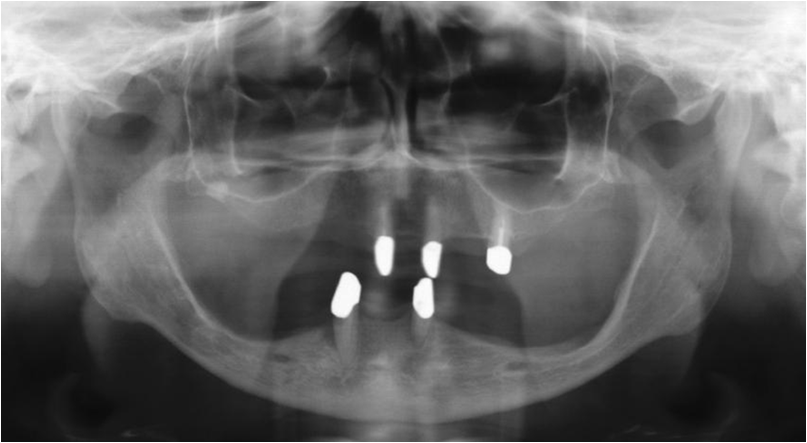
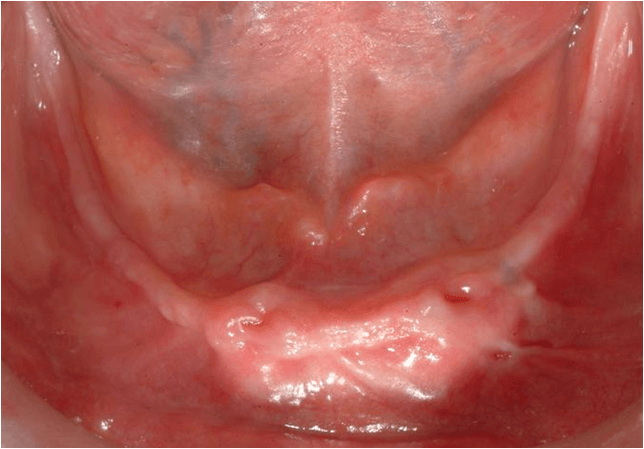
The treatment of the edentulous jaw can be a mixture of placing implants in healed and fresh extraction sockets. Unequal hard and soft tissue levels around the implants (Fig. 1&2), especially in the interforaminal region, can be adjusted by leveling the bone to an equal level.
In short-term follow-up studies no difference between placing implants in fresh extraction sockets vs. healed sockets was found. Recent literature shows that immediate implant placement combined with immediate loading does also not decrease survival rates of implants.
Immediate implant placement in fresh extraction sockets cannot prevent resorption of the alveolar crest. An advantage of immediate placement of implants is however the preservation to a certain extent of the peri-implant soft tissue (Fig. 3). After 2 years peri-implant bone resorption rates of implants placed in fresh extraction vs. healed sockets are similar.

Implants in healed extraction sockets
Advantages:
- Resolution of possible infections
- Healing of bone defects
- Increased soft tissue volume generated by soft tissue healing of the extraction socket
Disadvantages:
- Progressive reduction of bone volume by continuing alveolar ridge resorption
- Extended treatment time
Implants in fresh extraction sockets
Advantages:
- Reduction of total treatment time
- Reduction of patients’ discomfort
Disadvantages:
- Primary stability may be compromised
- Volume of keratinised mucosa on buccal/lingual site implant may be compromised