-
0
Patient Assessment
- 0.1 Patient demand
- 0.2 Overarching considerations
- 0.3 Local history
- 0.4 Anatomical location
- 0.5 General patient history
-
0.6
Risk assessment & special high risk categories
- 5.1 Risk assessment & special high risk categories
- 5.2 age
- 5.3 Compliance
- 5.4 Smoking
- 5.5 Drug abuse
- 5.6 Recreational drugs and alcohol abuse
- 5.7 Parafunctions
- 5.8 Diabetes
- 5.9 Osteoporosis
- 5.10 Coagulation disorders and anticoagulant therapy
- 5.11 Steroids
- 5.12 Bisphosphonates
- 5.13 BRONJ / ARONJ
- 5.14 Radiotherapy
- 5.15 Risk factors
-
1
Diagnostics
-
1.1
Clinical Assessment
- 0.1 Lip line
- 0.2 Mouth opening
- 0.3 Vertical dimension
- 0.4 Maxillo-mandibular relationship
- 0.5 TMD
- 0.6 Existing prosthesis
- 0.7 Muco-gingival junction
- 0.8 Hyposalivation and Xerostomia
- 1.2 Clinical findings
-
1.3
Clinical diagnostic assessments
- 2.1 Microbiology
- 2.2 Salivary output
-
1.4
Diagnostic imaging
- 3.1 Imaging overview
- 3.2 Intraoral radiographs
- 3.3 Panoramic
- 3.4 CBCT
- 3.5 CT
- 1.5 Diagnostic prosthodontic guides
-
1.1
Clinical Assessment
-
2
Treatment Options
- 2.1 Mucosally-supported
-
2.2
Implant-retained/supported, general
- 1.1 Prosthodontic options overview
- 1.2 Number of implants maxilla and mandible
- 1.3 Time to function
- 1.4 Submerged or non-submerged
- 1.5 Soft tissue management
- 1.6 Hard tissue management, mandible
- 1.7 Hard tissue management, maxilla
- 1.8 Need for grafting
- 1.9 Healed vs fresh extraction socket
- 1.10 Digital treatment planning protocols
- 2.3 Implant prosthetics - removable
-
2.4
Implant prosthetics - fixed
- 2.5 Comprehensive treatment concepts
-
3
Treatment Procedures
-
3.1
Surgical
-
3.2
Removable prosthetics
-
3.3
Fixed prosthetics
-
3.1
Surgical
- 4 Aftercare
Hard tissue management - mandible
Key points
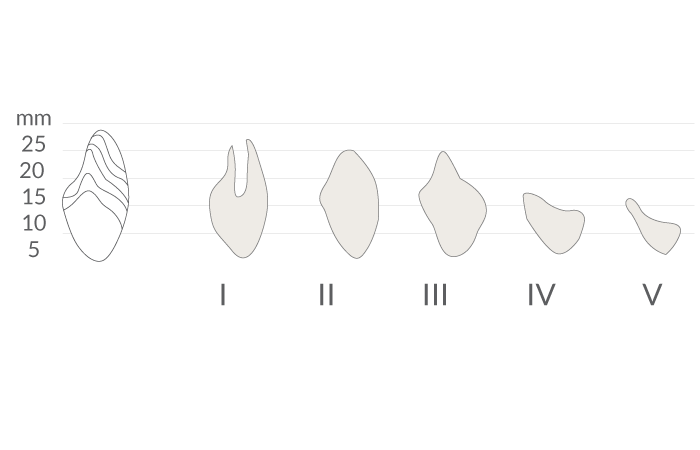
- Tooth extraction is followed by atrophy of the hard and adjacent soft tissues
- Insufficient amount of bone requires augmentation procedures
- Bone or different bone substitute materials can be used for augmentation procedures
The scientific literature shows that short implants with a length of ≥ 6 mm are able to support prosthetics in the edentulous mandible. After tooth removal the mandible displays different degrees of atrophy (Fig 1&2). Regarding hard tissue management one has to decide which regions of the mandible are affected. The interforaminal region of the mandible often offers an adequate bone height to insert dental implants...

Treatment options for vertical deficiency
- Grafting (with autogenous bone, freezed-dried bone, or bone substitute material)
- Osteotomy (with interposition of bone or bone substitute material)
- Distraction osteogenesis. After osteotomy a distraction device is inserted temporary and the two segments are moved apart until the desired distraction height is achieved
- Lateralization of the mandibular nerve

Treatment options for horizontal deficiency
- Grafting (with autogenous bone or bone substitute material)
- Ridge splitting (horizontal width is increased with chisels followed by an osteotome or bone expander before implant insertion)
- Leveling of the bone (if horizontal dimension allows this procedure)
To achieve maximal protection of the mandibular nerve pre-implant imaging (3D Imaging tools) are helpful to clearly identify the position of the mandibular canal (Fig 4).

Clinical topics
Additional resources

Questions
Ask a question
Log in or sign up to continue
You have reached the limit of content accessible without log in or this content requires log in. Log in or sign up now to get unlimited access to all FOR online resources.
No payments necessary - FOR is completely free of charge.