-
0
Patient Assessment
- 0.1 Patient demand
- 0.2 Overarching considerations
- 0.3 Local history
- 0.4 Anatomical location
- 0.5 General patient history
-
0.6
Risk assessment & special high risk categories
- 5.1 Risk assessment & special high risk categories
- 5.2 age
- 5.3 Compliance
- 5.4 Smoking
- 5.5 Drug abuse
- 5.6 Recreational drugs and alcohol abuse
- 5.7 Parafunctions
- 5.8 Diabetes
- 5.9 Osteoporosis
- 5.10 Coagulation disorders and anticoagulant therapy
- 5.11 Steroids
- 5.12 Bisphosphonates
- 5.13 BRONJ / ARONJ
- 5.14 Radiotherapy
- 5.15 Risk factors
-
1
Diagnostics
-
1.1
Clinical Assessment
- 0.1 Lip line
- 0.2 Mouth opening
- 0.3 Vertical dimension
- 0.4 Maxillo-mandibular relationship
- 0.5 TMD
- 0.6 Existing prosthesis
- 0.7 Muco-gingival junction
- 0.8 Hyposalivation and Xerostomia
- 1.2 Clinical findings
-
1.3
Clinical diagnostic assessments
- 2.1 Microbiology
- 2.2 Salivary output
-
1.4
Diagnostic imaging
- 3.1 Imaging overview
- 3.2 Intraoral radiographs
- 3.3 Panoramic
- 3.4 CBCT
- 3.5 CT
- 1.5 Diagnostic prosthodontic guides
-
1.1
Clinical Assessment
-
2
Treatment Options
- 2.1 Mucosally-supported
-
2.2
Implant-retained/supported, general
- 1.1 Prosthodontic options overview
- 1.2 Number of implants maxilla and mandible
- 1.3 Time to function
- 1.4 Submerged or non-submerged
- 1.5 Soft tissue management
- 1.6 Hard tissue management, mandible
- 1.7 Hard tissue management, maxilla
- 1.8 Need for grafting
- 1.9 Healed vs fresh extraction socket
- 1.10 Digital treatment planning protocols
- 2.3 Implant prosthetics - removable
-
2.4
Implant prosthetics - fixed
- 2.5 Comprehensive treatment concepts
-
3
Treatment Procedures
-
3.1
Surgical
-
3.2
Removable prosthetics
-
3.3
Fixed prosthetics
-
3.1
Surgical
- 4 Aftercare
Flap or flapless
Key points
- In the mandible, measure the distance from the alveolar crest to the mandibular canal and to the mental foramina
- In the maxilla, measure the distance from the alveolar crest to the maxillary sinus
- Measure the distance from the mucosal margin to the alveolar crest in mm
- A minimum of 4 mm of buccal-lingual width at the alveolar crest is necessary
- It is optional to measure the width of keratinized mucosa
- Use the precision drill for initial penetration through mucosa into alveolar bone
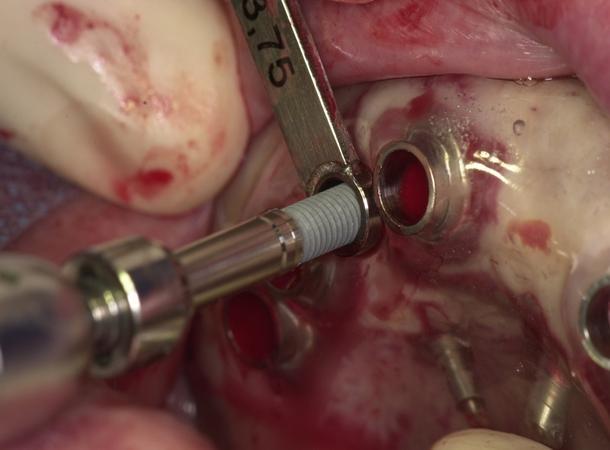
Flapless Implant Placement
Flapless implant surgery is a minimally invasive procedure that can be performed either using guided surgery or custom fabricated surgical guides made of casts taken at the first patient visit. Several clinical papers reported excellent short- and long-term survival rates for implants placed using flapless or minimally invasive approaches.
Flapless implant placement, under appropriate conditions, is a rewarding procedure for patients. There is minimal bleeding and postoperative discomfort with excellent implant survival rates (98.7% at 2 years). These procedures, when applicable, provide patients and doctors with another treatment approach. A surgical guide is fabricated from the cast made at the initial visit. Prior to surgery patients are usually placed on a prophylactic antibiotic regimen. Choice of antibiotics is usually dictated by the patient’s health history and consideration of potential allergies. Patients can be sedated orally or intravenous conscious sedation can be used to allay patients’ fears. Local-regional anesthesia is performed in any case. Pre-surgery patients rinse with a chlorhexidine rinse. The surgical site is swabbed with an antiseptic.
The surgical guide is positioned and a periodontal probe is used to measure the distance from the occlusal aspect of the mucosal margin to the alveolar crest. This is an important measurement. If the preplanned implant size is 4.3 mmx11.5 mm and the measured depth from the mucosal margin to the alveolar crest is 3 mm, the site should be prepared to a depth of 14.5 mm (11.5 mm+3 mm=14.5 mm). The precision drill can then be used to perform the initial osteotomy. The 2 mm drill follows to the appropriate depth. The drill is disengaged from the handpiece, left in place and a test radiograph is taken to evaluate implant angulation and depth. Site preparation is completed and the appropriate implant is installed into the osteotomy. A healing abutment is placed into the implant. In most instances suturing is not necessary. Resonance Frequency Measurement can be performed prior to the insertion of the healing abutment; this step is optional. Healing is evaluated after one week and again after an appropriate healing interval (3-4 months). At the date of evaluation of the implant integration, the healing abutment is removed and the resonance frequency measurements are recorded. The site is evaluated for implant stability, peri-implant bone levels, soft tissue levels and their condition (no inflammation) and the patient is ready for implant restoration.
The restorative dentist or prosthodontist has several options: from impression-taking and using custom abutment/retention elements to the use of pre-fabricated stock abutments/retention elements. The restorative doctor makes the restorative choices. Ideally, for fixed solutions, the final restoration should be screw-retained. Once the restoration has been placed and the occlusion has been evaluated, the patient should be placed into a maintenance program including periodontal, functional and prosthetic evaluation. The implant should be evaluated for stability; mobility and a periapical radiograph should be taken annually.
Courtesy of Dr. Daniel van Steenberghe, Brussels
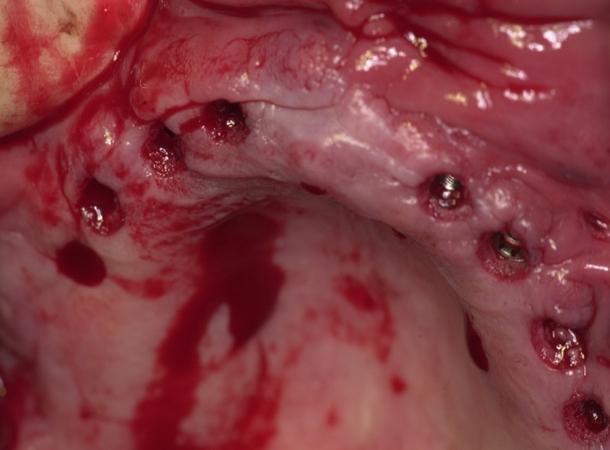
Courtesy of Dr. Daniel van Steenberghe, Brussels
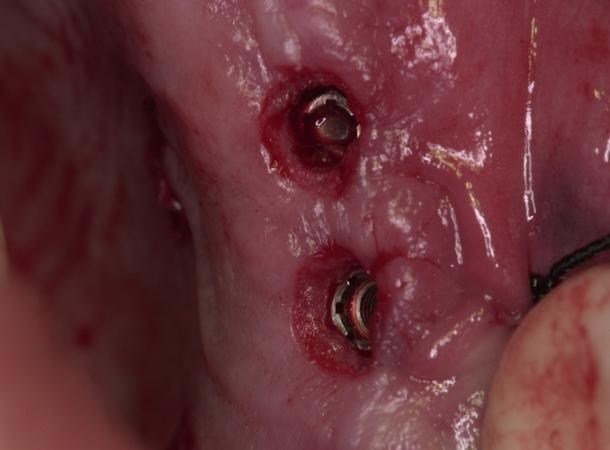
Courtesy of Dr. Daniel van Steenberghe, Brussels
Flap procedures
Note: All flap procedures are open.
Consider flap procedures:
- to visualize crestal bone
- in situations with a narrow alveolar ridge, insufficient keratinized mucosa and to maintain keratinized tissue
- in anticipation of the need for tissue augmentation/sinus augmentation
- for esthetic reasons
In situations where there is insufficient keratinized mucosa, a flap can be raised, thereby preserving the keratinized mucosa. A free gingival graft can also be considered in order to increase the dimension of keratinized tissue.
Considerations
For the treatment planning, evaluate patient's general and local histories, periapical and panoramic radiographs, study casts, interocclusal space, patient's mouth opening, clinical photographs, ridge mapping (intraorally and on study casts), the surgical guide made on study cast.
Consider computerized tomography if vital structures and bone height and width cannot be determined through periapical or panoramic radiographs.



