Maxillary Anterior Immediate Tooth Replacement with Socket-Shield Technique
The patient, a healthy 78-year-old male, presented with a failing maxillary left central incisor (tooth #9). Clinical examination revealed extensive caries compromising the long-term prognosis of the tooth. Despite the structural compromise, the tooth presented no signs of mobility, pathology, or subcrestal fracture, allowing thoughtful consideration of immediate implant therapy.
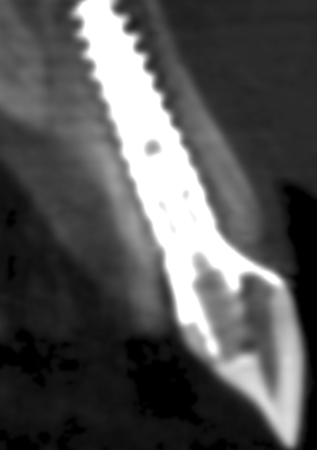
Radiographically, the facial bone plate was intact and sufficient bone volume was present to support immediate implant placement. The periodontal tissues showed no signs of active infection, and the soft-tissue phenotype was favorable for an esthetic anterior-zone rehabilitation. These findings supported the feasibility of applying the Socket-Shield technique (Publication 1) to preserve the facial contour.
The patient expressed clear restorative goals: a fixed solution (preferably implant-supported), closure of the diastema between the maxillary central incisors, and avoidance of any removable provisional during healing. His expectations, combined with the favorable clinical and anatomical findings, guided the decision toward Immediate Implant Placement and Provisionalization (IIPP) with a Socket-Shield approach.
Evaluation & Diagnosis

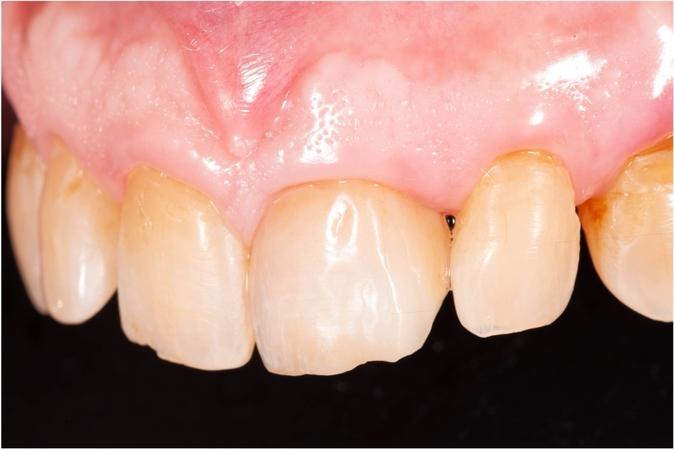
Smile view

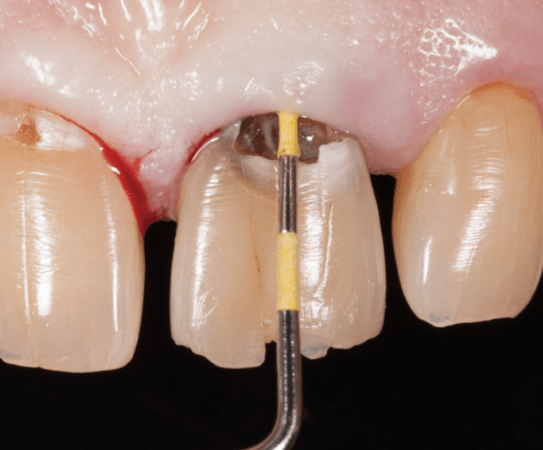
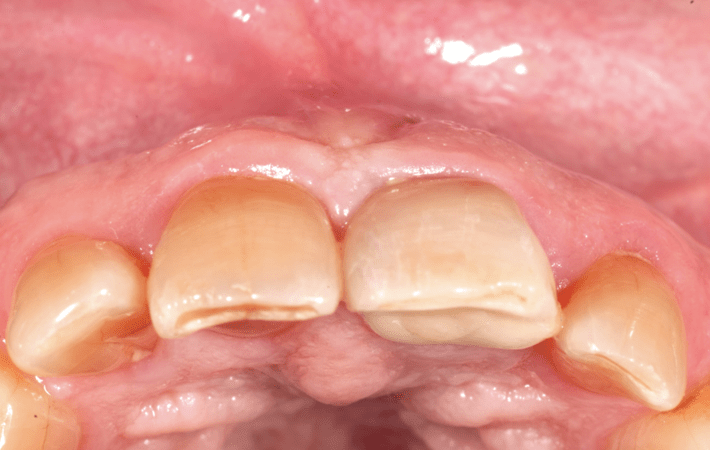
Facial view of the deep cavitated left central incisor

Incisal view of failing left central incisor


Treatment Planning
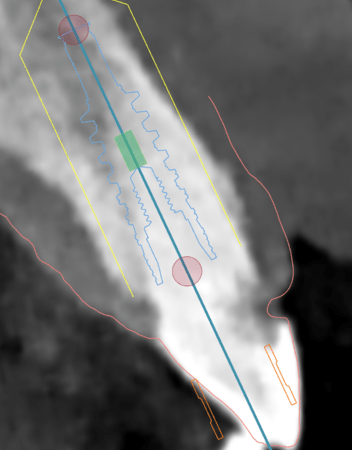
Treatment planning began with confirmation that the case was suitable for IIPP with maintenance of the facial root fragment. The presence of intact facial bone and sufficient apical anchorage permitted planning implant placement approximately 4 mm apical to the pre-determined facial mucosal margin. This apico-coronal positioning was critical for achieving an optimal esthetic emergence profile.
A comprehensive plan was developed that included creating a 1 mm gap between the implant and the retained facial root segment (Socket-Shield, SS) and filling this space with a 50:50 blend of mineralized allograft (Creos™ allo.gain) and xenograft (Creos™ xenogain). These biomaterials were selected to support long-term contour preservation, ensure space maintenance, and provide consistent regenerative potential (publication 2).
The definitive restorative plan included an Angulated Screw Channel (ASC) abutment with a zirconia-based restoration to optimize esthetics and screw-retained retrievability. The provisional phase would involve a relined shell restoration adjusted to avoid all functional contacts, enabling safe and predictable osseointegration during the four-month healing period.
Progress & Completion
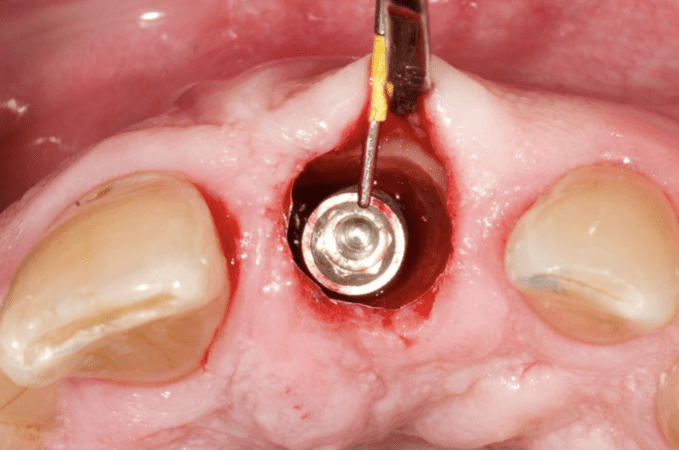
Incisal view showing the prepared socket shield and a gap between the root shield and the implant platform
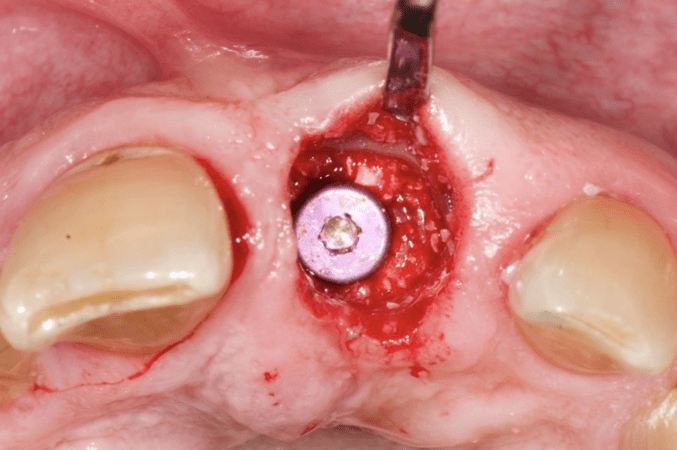
Placement of a mixed allograft and xenograft bone graft particles in a 50:50 ratio mixture in the gap.

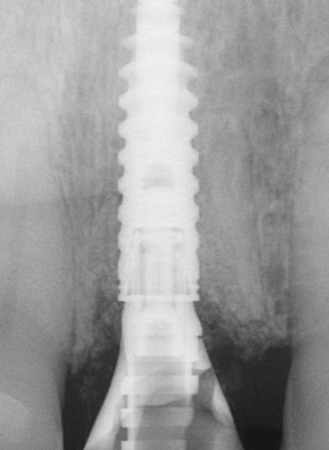
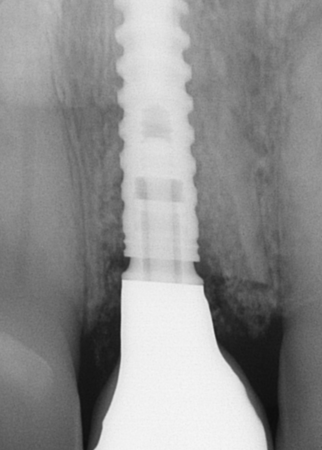
Periapical radiograph taken after surgery with retained socket-shield and provisional crown

Facial view at 1y follow-up before the placement of the definitive crown


One-year follow-up with the definitive implant-supported crown on the left central incisor.
The Socket-Shield (SS) was prepared by initially sectioning the failing root mesio-distally. Subsequently, the palatal root portion was atraumatically removed using an elevator. The residual facial root fragment was then adjusted with a diamond bur to create a 1-1.5 mm thick, C-shaped SS (publication 3). The SS extended from the mesial to the distal interproximal line angles of the socket. Finally, the coronal portion of the SS was adjusted to the level of the facial bone crest, incorporating a palatal bevel directed towards the central region of the tooth socket (media 8,14,15).
After careful root sectioning and preparation of the SS, sequential osteotomies were performed to achieve ideal 3D implant positioning. A NobelActive 3.5 × 15 mm implant was inserted with an insertion torque exceeding 25 Ncm, providing adequate primary stability for immediate provisionalization. A >1 mm gap was left between the implant and the facial SS (Publication 2). The graft mixture was placed meticulously around the shield–implant gap and extended coronally to support the soft-tissue architecture.
A provisional crown was fabricated by relining a shell restoration and securing it to a temporary abutment. The provisional was screw-retained, designed with no centric or eccentric contacts, and hand-tightened to protect the implant during the osseointegration phase. The patient was instructed to maintain a soft diet and follow strict oral hygiene recommendations during the healing period.
One year after implant placement, the final restoration was delivered. A screw-retained all-ceramic crown (VITA VM13) supported by an ASC abutment was torqued to 35 Ncm according to manufacturer guidelines. The final esthetic result successfully closed the diastema, harmonized the smile line, and provided a natural soft-tissue emergence profile.
Follow-up & Outcome

4-year follow-up with the definitive implant-supported crown on the left central incisor.
4-year follow-up with the definitive implant-supported crown on the left central incisor

Smile view at four-year follow-up with the definitive implant-supported crown on the left central incisor.
4-year follow-up with the definitive implant crown.
Facial view at four-year follow-up showing facial mucosal profile was still well-maintained

3D rendering image occlusal
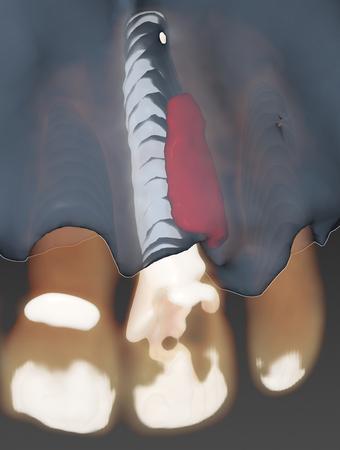
3D rendering image with Socket Shield
Postoperative healing was uneventful, with the patient reporting no discomfort or complications throughout the treatment sequence. Soft-tissue maturation progressed predictably, and the provisional restoration maintained the peri-implant mucosal contour during the critical healing phase. Oral hygiene compliance remained consistently high, contributing positively to the clinical outcome.
Follow-up examinations continued annually, providing the opportunity to monitor peri-implant stability and soft-tissue integrity. At the four-year follow-up, both clinical and radiographic evaluation demonstrated stable peri-implant bone levels, healthy soft tissues, and an intact facial mucosal profile. The implant restoration remained functional and esthetically harmonious with the adjacent dentition.
This case underscores the importance of correct case selection and precise surgical execution when performing IIPP combined with the Socket-Shield technique. The successful long-term outcome aligns with recent literature suggesting that socket-shield approaches may enhance preservation of the facial mucosal profile compared with IIPP alone (Publication 2). The treatment fulfilled the patient’s esthetic and functional expectations while avoiding removable provisionalization entirely.
Discussion
Careful case selection is essential for the success of this technique, with specific exclusion criteria recommend:
Patient who:
- (1) is smoker and/or using electronic cigarettes and/or other forms of nicotinic products
- (2) has a history of bruxism and/or severe parafunctional habits,
- (3) has untreated periodontal disease,
- (4) lacks stable posterior occlusion,
- (5) has compromised facial bone, mobility, pathology or subcrestal root fracture of the failing tooth
- (6) has compromised implant and/or SS stability during the surgery, and/or
- (7) has SS less than 6 mm height after preparation (Publication 2).
The length and width of the SS should also be taken into consideration. A recent published 1- to 10-Year retrospective study suggests preparing the occlusal SS as C-shaped to prevent interproximal exposure (Publication 3, illustrated in the current case. Media 14,16). The SS should be a minimum of 6mm in length (Publication 2, Media 15,16). Overpreparing SS may result in weaking its structure, and prone to mobility (Reference 4).
Conclusion
With proper case selection and careful surgical implementation, including precise implant positioning and grafting procedures (Publication 2), Immediate implant placement and provisionalization (IIPP) with socket-shield technique can be a viable treatment option for esthetic demanding patients.







Why was the implant not centered on the space. It is a very nice case but it appears that the restoration had less than ideal co
In reply to Why was the implant not centered on the space. It is a very nice case but it appears that the restoration had less than ideal co by Sean Bradley
Thank you for your question!
The off-center placement was actually intentional. The patient wanted to close his midline diastema. I strategically positioned the implant mesially to create the proper emergence profile for that closure, which required shifting the implant away from the center of the socket while preserving the facial & distal Socket-Shield (SS).