Use of implant anchorage to correct an anterior cross bite in a patient with a class III malocclusion. A Case Report
A 62-year old male patient was referred by their long-time restorative dentist with a chief complaint, “I want to restore my entire mouth. Everything is breaking, my bite is off, and I can’t seem to chew properly”. He has a history of sleep apnea, a strong gag reflex, and an inability to keep his throat closed during dental treatment. His past dental history included extensive restorative treatment with porcelain fused to metal crowns and resin restorations.
Extraorally, there is a limited range of maximal opening, however, TMJs were asymptomatic. No lymph node swellings were noticed around the neck and chin area. Facial skin, nose, and lips were all healthy.
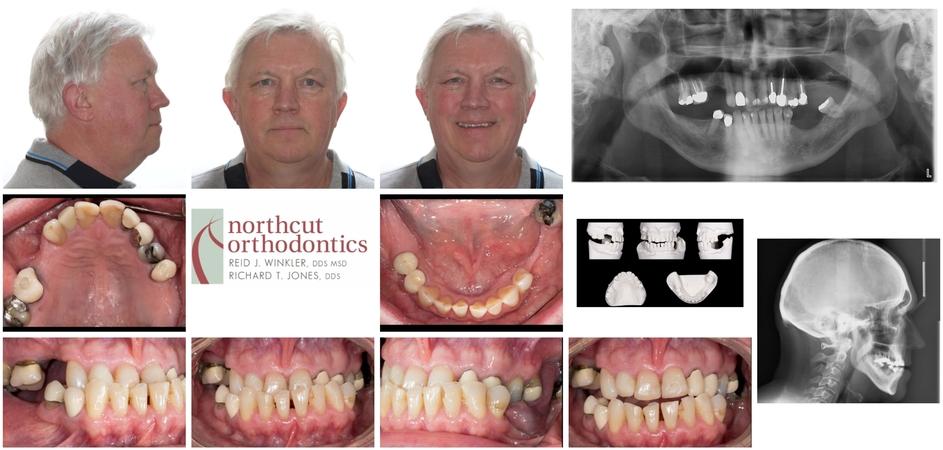
Intraorally, there is a skeletal/dental class III malocclusion with an anteroposterior crossbite, multiple missing posterior teeth, ill-fitting restorations, generalized dental caries, occlusal interferences in protrusive and lateral excursive movements. In addition, we noticed extensive occlusal wear, a reverse occlusal plane, diastemata in lower anteriors, multiple resin restorations, and generalized 1-2mm mobility with reduced periodontal support.
The challenge, in this case, was to reset the occlusion and restore the entire mouth, given the very few posterior dentitions and compromised periodontal support.
Evaluation & Diagnosis

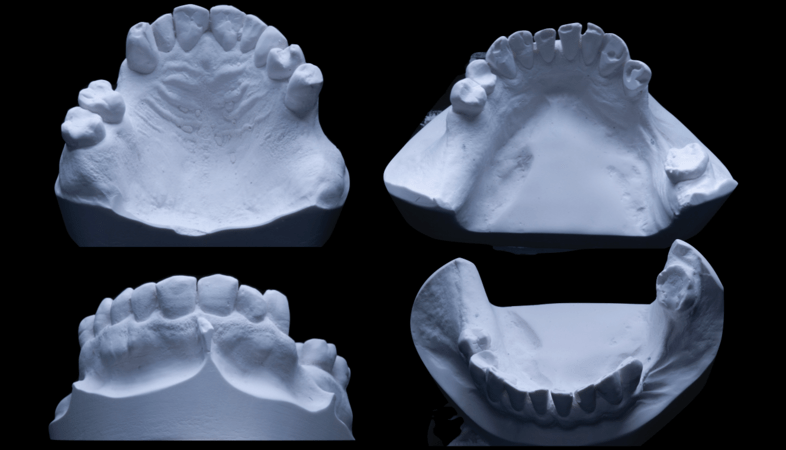
Initial situation showing a class 3 malocclusion, anterior cross bite and uneven occlusal planes.







A 62-year-old male patient was referred by their long-time restorative dentist with a chief complaint, “I want to restore my entire mouth. Everything is breaking, my bite is off, and I can’t seem to chew properly”. He has a history of sleep apnea, a strong gag reflex, and an inability to keep his throat closed during dental treatment. His past dental history included extensive restorative treatment with porcelain fused to metal crowns and resin restorations.
Treatment Planning

A digital set up was done demonstrating that lower premolars needed to be retracted 3.5mm per side.
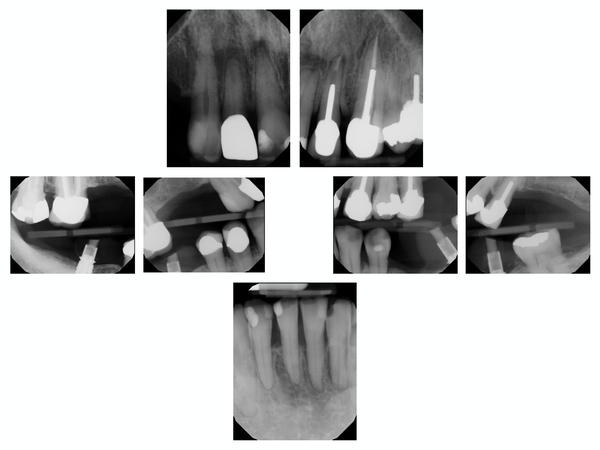
Note the peri apical radiolucencies 7,8,9 and 10, as well as the extensive dental restorations.
A digital set up was done demonstrating that lower premolars needed to be retracted 3.5mm per side. Space for #4/5 was enlarged to 14mm and space was created between #10/11 to advance the upper incisors. Conventional edgewise orthodontic mechanics were used with .022” slot MBT twin brackets. Brackets were bonded to implant provisionals. Treatment time was 22 months in braces.
Progress & Completion
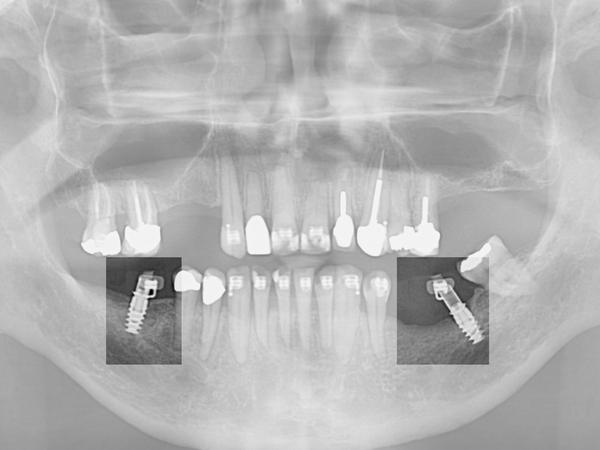
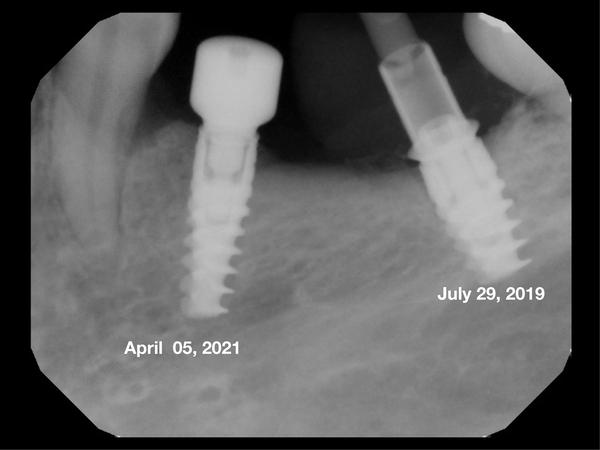
Radiograph with implant #19 and #30 placed July 29, 2019. Nobel Active implants to be used as orthodontic anchorage.
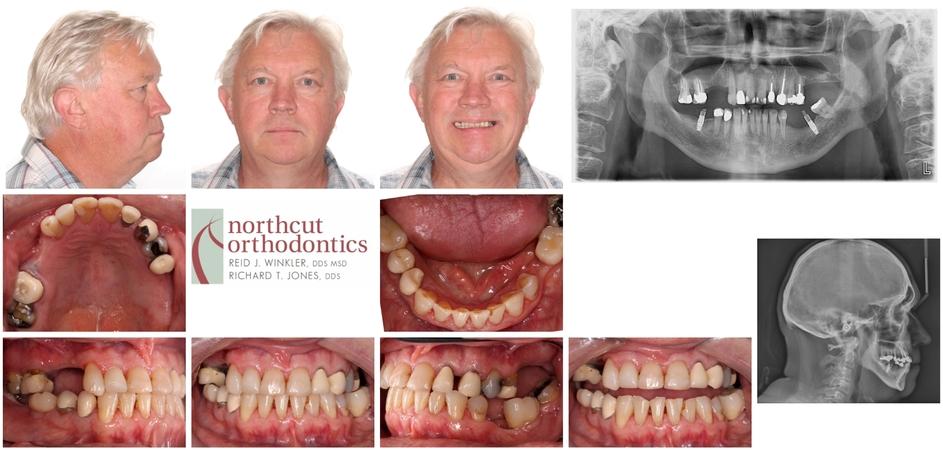

Post-ortho teeth alignment, anterior cross bite correction, and teeth positioning for future restorative work.

Vertical dimension was not changed due to patients difficulty of maximal opening established during the diagnostic exam.

Allows patient to visualize final prosthodontic treatment before it begins.

Vertical dimension of occlusion remained unchanged.

Set-up preparation guides to help visualize depth reduction.
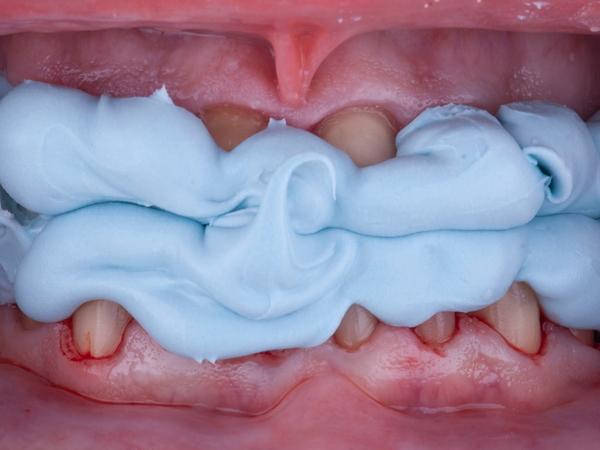
Interocclusal records following preps and impressions of both arches simultaneously.

Preparing both arches in these types of cases is imperative to facilitate a better control of the occlusion.

Shade matching different substrates/abutments was challange for the clinician and lab to control the esthetic outcome.

Double cord technique using a double zero (00) and zero (0) for tissue displacement.

A combination of screw retained implant crowns and Lithium disilicate veneers.

Restorations tried-in for fit before cementation. Cemented simultaneously, one arch at a time.

Meticulous excess cement removal, hence slight tissue irritation. It is key to maintaining long term tissue health.
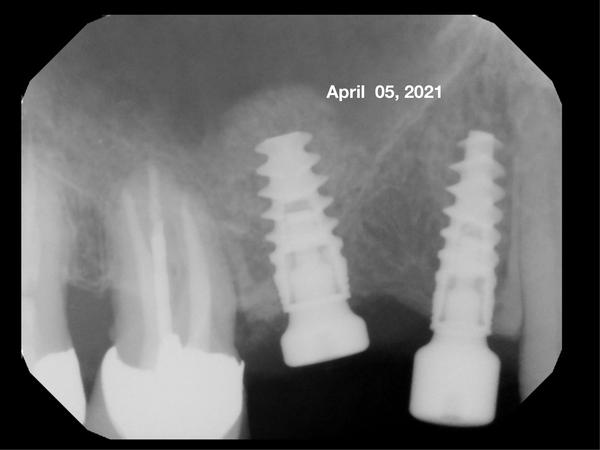
Post COVID, Nobel active implants placed in positions 4, 5, & 20. A trans-crestal sinus augmentation and simultaneous implant placement #4 (4.3X11.5mm). #5 (3.5X11.5mm), #20 (3.5X11.5mm) placed in April 05, 2021.
Post ortho teeth alignment, anterior cross bite correction, and teeth positioning for future restorative work. Implants #19 and #30 used for orthodontic anchorage. Conventional edgewise orthodontic mechanics were used with .022” slot MBT twin brackets. Brackets were bonded to implant provisionals. Treatment time was 22 months in braces.
Follow-up & Outcome

Six months post insertion showing stable healthy tissues.
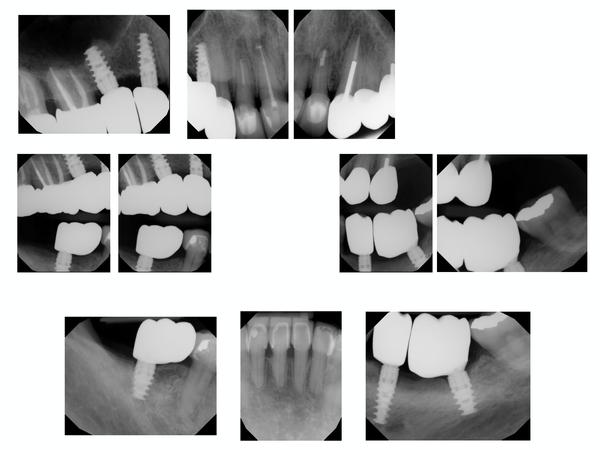
Periapical radiolucencies are mineralizing, implant bone levels remain stable.

Anterior guidance showing contact on the centrals and slightly lateral incisor.

Close-up smile six months post restorative treatment.


Mandibular occlusal view showing final restorations in-situ.

Maxillary occlusal view showing final restorations in-situ. The Zr copings helped to block-up the dark build-ups.
A comprehensive interdisciplinary treatment plan, prior to any extensive prosthodontic full mouth rehabilitation is highly recommended. In cases with complex orthodontic problems, endosseous dental implants placed in pre planned positions based on an orthodontic set-up, is key for optimum success. The difficulty in this case was the accurate placement of implants and the ortodontic correction of a skeletal class III using only a dental approach.

Was the patient deprogrammed first to access whether his maxilla-mand relationship was anteriorly displaced. How did you
If the vd was opened how much retrusion of the mandible could be attained. Lastly how did you monitor or evaluate sir volume changes as related to retraction of lowers and bicuspids. Thank you
If the vd was opened how much retrusion of the mandible could be attained. Lastly how did you monitor or evaluate sir volume changes as related to retraction of lowers and bicuspids. Thank you
In reply to Was the patient deprogrammed first to access whether his maxilla-mand relationship was anteriorly displaced. How did you by Anonymous
A deprogrammer was not used in this case, although it is one of many excellent approaches. Post orthodontics, a diagnostic wax up was fabricated and superimposed intra-orally to determine patient comfort at new VDO, thereafter which preparations and temporary restorations were fabricated.
In reply to Was the patient deprogrammed first to access whether his maxilla-mand relationship was anteriorly displaced. How did you by Anonymous
In my experience, patients with Class III skeletal pattern do not posture anteriorly. If there is a pre-treatment discrepancy between CR and MIP, it's typically an anterior first point of contact that causes the patient to slide into a reverse overjet relationship anteriorly. This is also the primary reason for wear and chipping of the anterior teeth for a Class III patient.
Class II patients, on the other hand, are the patients that more often will require deprogramming (in this case referring to pre-treatment orthosis, not an NTI, lucia jig, or leaf guage). I am a board certified prosthodontist, I also do not deprogram every patient, but I rely on the initial clinical exam, and in particular my ability to capture a centric record using bimanual manipulation (Dawson method). If there is any muscular incoordination or posturing detected, I will certainly include some type of orthosis or orthotic concept in their pre-treatment work-up. Orthosis I also find is the best way to test an increased OVD for a dentate or mostly dentate patient.
Beautiful case, Rich.
Regards,
R.
In reply to Was the patient deprogrammed first to access whether his maxilla-mand relationship was anteriorly displaced. How did you by Anonymous
Thank you for the very well organized and stimulating thought process on deprogramming in relation to this case and other skeletal discrepancies. I enjoyed reading it R.
In reply to Was the patient deprogrammed first to access whether his maxilla-mand relationship was anteriorly displaced. How did you by Anonymous
Hi to everyone.
i have a similar case with III skeletal class maloccusion. There was a discrepancy between CO and CR approx 2 mm (in CR it was edge-to-edge contact). After fixing pads on molars and premolars in CR, i've changed torques frontal teeth, counterclockwise rotation of occlusion plane.
After implants placement, in the final stage of prosthesis, i've created pure left anf right canine guidance. Hope you'll enjoy