Two Stage Implant Placement for a Failing Central Incisor with Ankylosis to Labial Bone Plate.
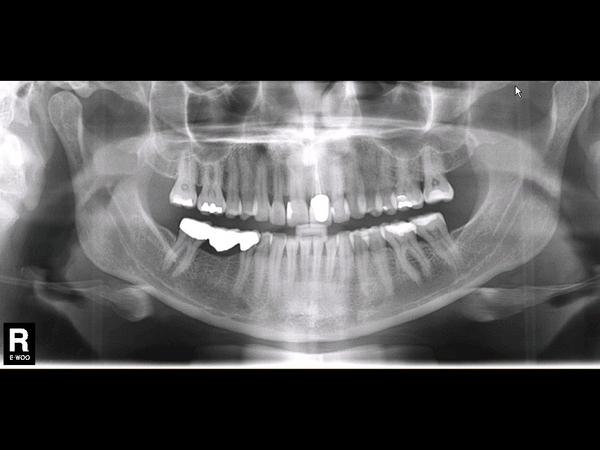
A 45-year-old female patient who was referred re-failing post crown in tooth #21 FDI (#9 US), multiple failed veneers, generalised tooth wear and loss of Occlusal Vertical Dimension (OVD). She was medically fit with No Relevant Medical Health (NRMH). In her dental diagnosis she presents generalised tooth wear and failing maxillary anterior restorations with multiple teeth needing restoration.
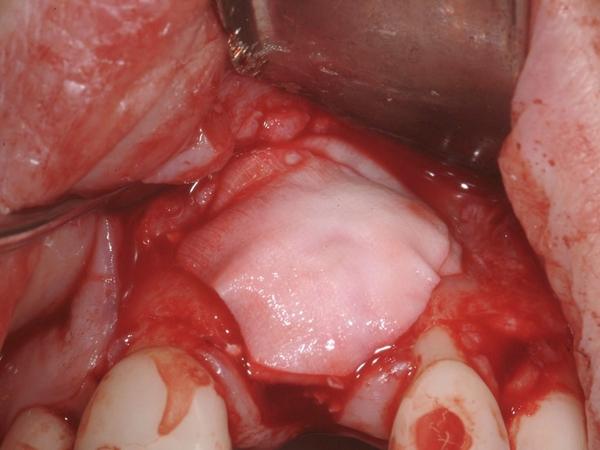
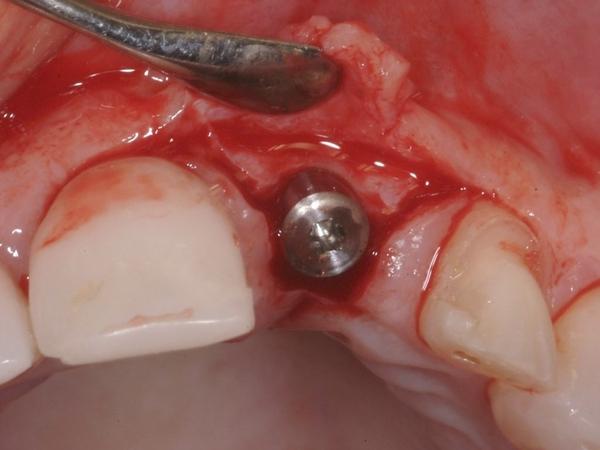
The treatment selected for the replacement of the central incisor involved the extraction of the root of #21 FDI (#9 US) initially hoping to carry out immediate implant placement, however ankylosis to labial bone plate necessitated delayed approach. The late-delayed two-stage implant (NobelActive®) was placed at 8 weeks with simultaneous Guided Bone Regeneration (GBR). On a second stage surgery at approximately 4 months with simultaneous soft tissue augmentation with a Connective Tissue (CT) graft was needed.
The prosthetic treatment selected for its first provisional was a Rochette fixed partial denture. Once the implant was placed, its provisional was made on a NobelProcera® Abutment Zirconia MZ and the final restoration was an IPS e.max® Lithium Disilicate crown on the zirconia abutment, along with the restoration of numerous upper and lower teeth.
Evaluation & Diagnosis




Treatment Planning






Progress & Completion


























Follow-Up & Outcome





Questions
Ask a questionCan you please post, clinical descriptions, documentation (photos) of the phase1 ... extraction... extent of, or topografi
The treatment selected for the replacement of the central incisor involved the extraction of the root of #21 FDI (#9 US) initially hoping to carry out immediate implant placement, however ankylosis to labial bone plate necessitated delayed approach.
***************************
First of all, thank you for sharing and congratulations on your achieving such an enjoyable presentation. This, in my opinion, is an humble but simple example for a Fantastic, Magnificent, Marvelous, most Admirable, and quite an ACHIEVABLE result for a proud profession excellence.
Most importantly,
The best ACHIEVED in our services "offers the most benefits" to our beloved patients... DOE IT????
**********************************
Now, comments:
1. It appears, that the first stage surgery...
Extract and graft procedure/s resulted in less than desired "RIDGE" contours... am I wrong?
A. What can we learn from this experience, of having to correct the "deficient ridge" yet.
B. What would you do different, to achieve even better, or best possible results!
C. What Is/was that compromised result (if it is) pointing to LEARN FROM, could it be
(I) Methods/procedure adopted, (ii) Materials used and or (iii) It just happens!!!
2. Could I be wrong, to point that a slightly more palatal positioning (A-P axial orientation) of implant plat form would have accommodated a nicer screw retained (crown) restoration?
3. Is it beneficial, if we were to design and create/prep a custom ABUTMENT with an accentuated axial, anti-rotational mechanical features to counter the potential functional failure of cements used?
Anti-rotational feature compliments cement's breakage resistance... does it? (#30,#46)
4. How was the lost Vertical Dimension of Occlusion was regained and restored? your procedural steps?
Thanks for listening,
Ashwath M Gowda. BDS., DDS., FAGD.
The treatment selected for the replacement of the central incisor involved the extraction of the root of #21 FDI (#9 US) initially hoping to carry out immediate implant placement, however ankylosis to labial bone plate necessitated delayed approach.
***************************
First of all, thank you for sharing and congratulations on your achieving such an enjoyable presentation. This, in my opinion, is an humble but simple example for a Fantastic, Magnificent, Marvelous, most Admirable, and quite an ACHIEVABLE result for a proud profession excellence.
Most importantly,
The best ACHIEVED in our services "offers the most benefits" to our beloved patients... DOE IT????
**********************************
Now, comments:
1. It appears, that the first stage surgery...
Extract and graft procedure/s resulted in less than desired "RIDGE" contours... am I wrong?
A. What can we learn from this experience, of having to correct the "deficient ridge" yet.
B. What would you do different, to achieve even better, or best possible results!
C. What Is/was that compromised result (if it is) pointing to LEARN FROM, could it be
(I) Methods/procedure adopted, (ii) Materials used and or (iii) It just happens!!!
2. Could I be wrong, to point that a slightly more palatal positioning (A-P axial orientation) of implant plat form would have accommodated a nicer screw retained (crown) restoration?
3. Is it beneficial, if we were to design and create/prep a custom ABUTMENT with an accentuated axial, anti-rotational mechanical features to counter the potential functional failure of cements used?
Anti-rotational feature compliments cement's breakage resistance... does it? (#30,#46)
4. How was the lost Vertical Dimension of Occlusion was regained and restored? your procedural steps?
Thanks for listening,
Ashwath M Gowda. BDS., DDS., FAGD.

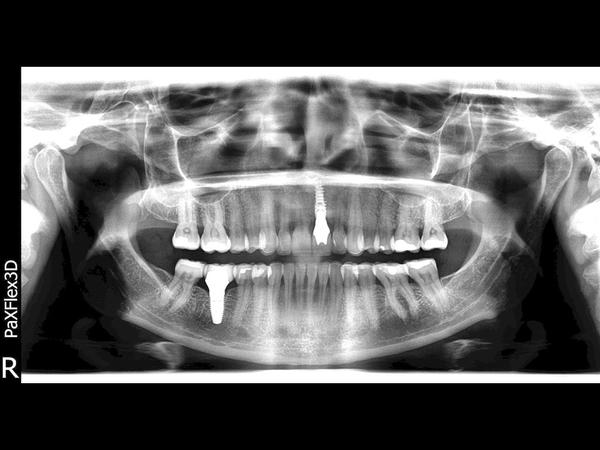
Is it possible to not show the text in front of the radiography
... as it doesn’t permit to see the image well
... as it doesn’t permit to see the image well
In reply to Is it possible to not show the text in front of the radiography by Daniel Sandor
Thank you very much for bringing this to our attention. We looked into the issue and noticed that the current implementation of text is not optimal for all images across the entire website (when accessing on a mobile device). We will fix this as soon as possible. Thank you, Joel from FOR