Stackable Guide and Staged Planning for Full Mouth Rehabilitation
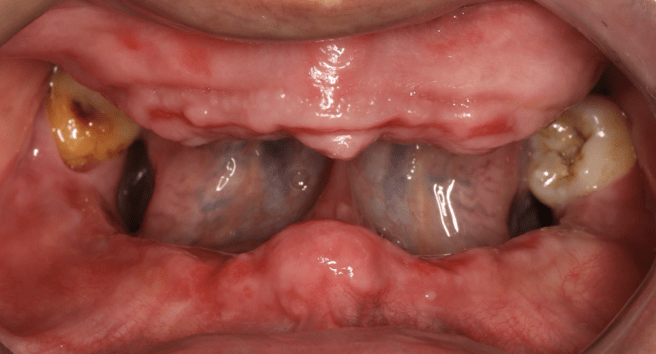
A 45-year-old male patient diagnosed with generalized severe periodontitis, classified as Stage IV, Grade C, characterized by extensive infection, compromised dentition, and significant functional instability. The pre-therapeutic prognosis revealed that a large number of teeth were considered irrational to treat or of doubtful prognosis, leading to the indication for full-mouth rehabilitation.
Due to the severity of the condition, including mandibular instability and loss of vertical dimension of occlusion (VDO), a comprehensive and staged treatment approach was required. The treatment plan involved full-mouth extraction followed by delayed implant placement, combined with the use of interim and provisional prostheses to progressively restore function and aesthetics.
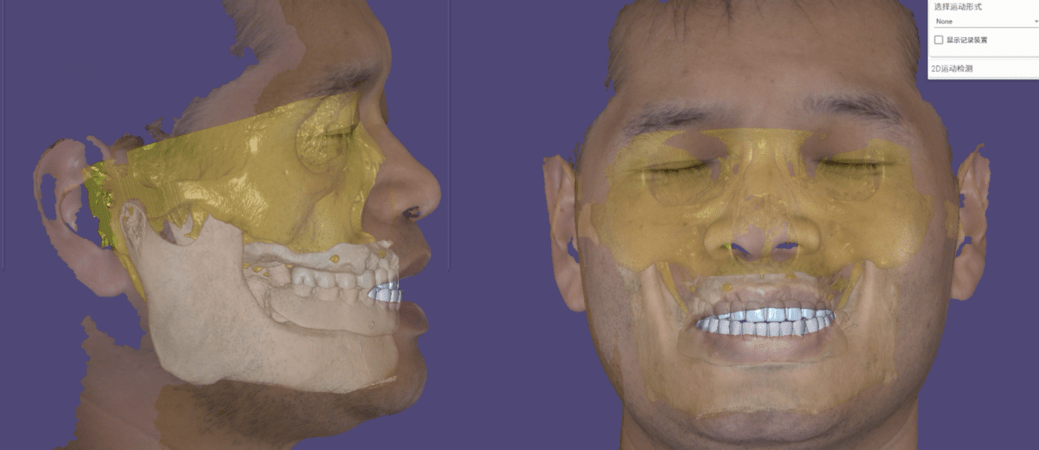
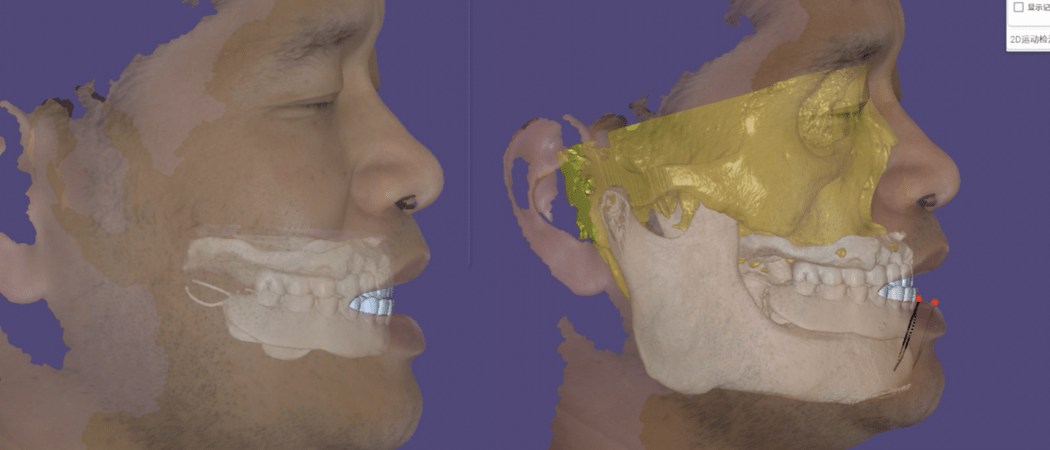
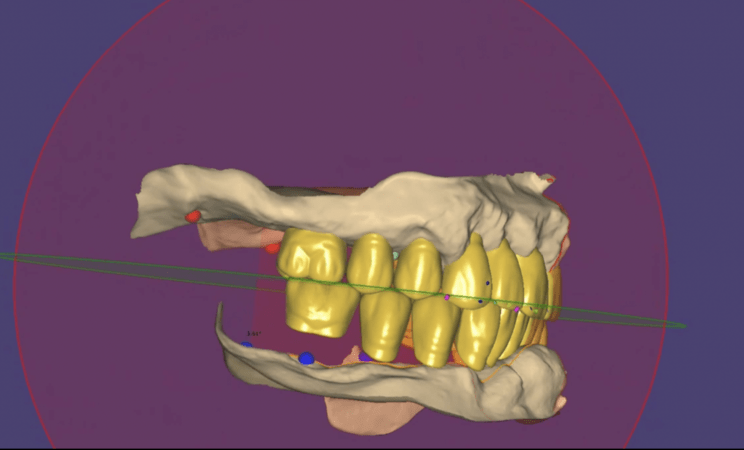
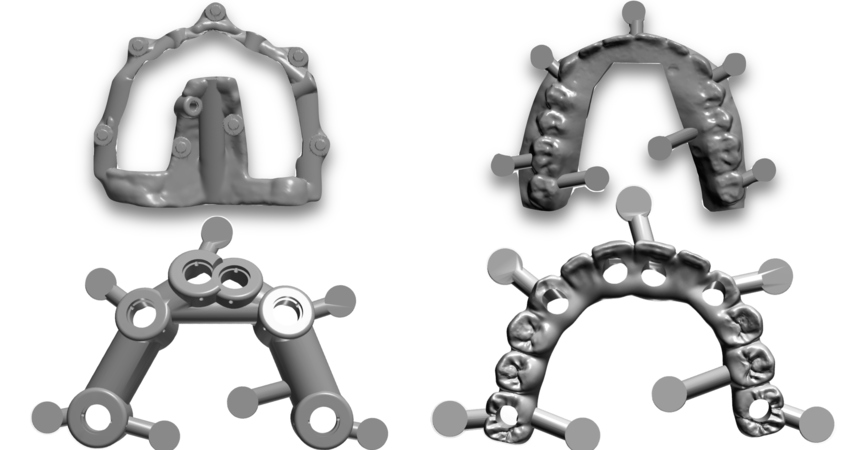
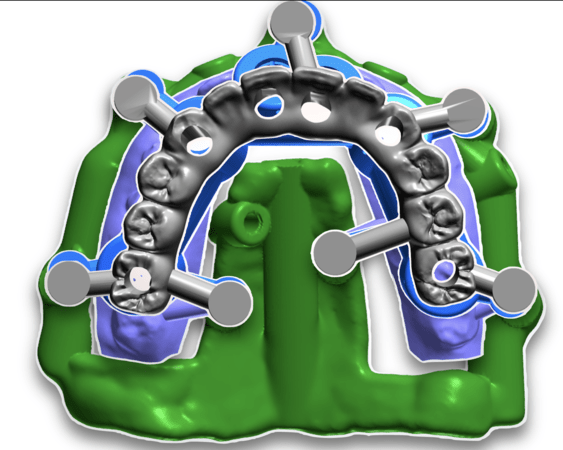
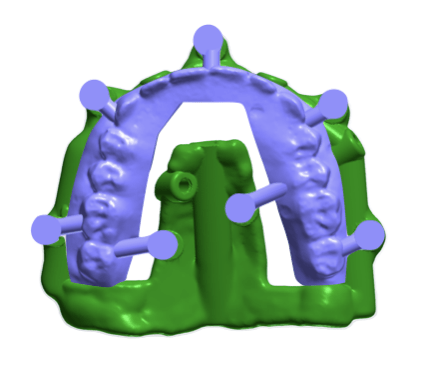
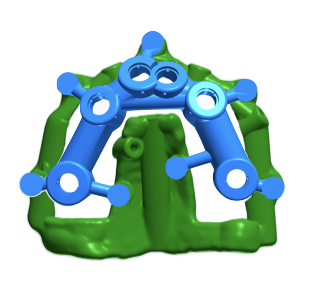
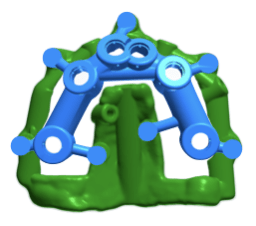
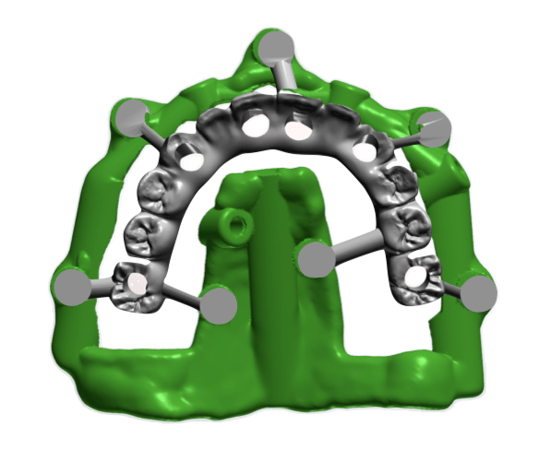
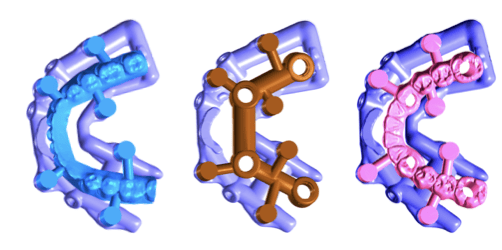
A key aspect of this case was the integration of digital workflows, including a “virtual patient” concept and the use of stackable surgical guides, allowing for precise implant positioning and prosthetic planning. The staged increase in VDO and continuous functional evaluation enabled a predictable transition from an unstable oral condition to a definitive implant-supported full-mouth rehabilitation.
Evaluation & Diagnosis

Presented with chief complaints of the teeth mobility, poor aesthetics, and pain during mastication.

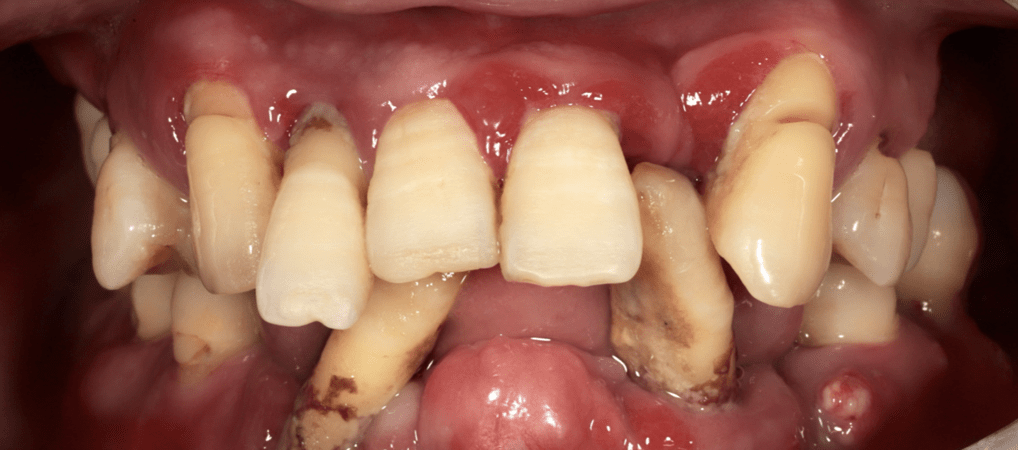
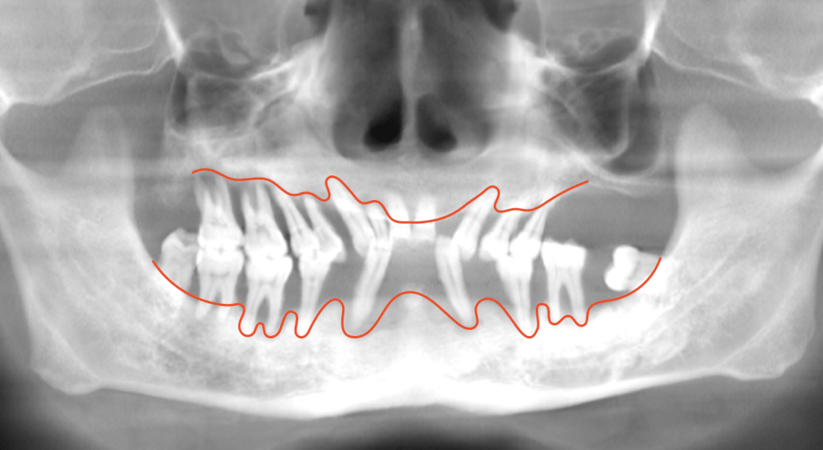
Partially edentulous dentition with generalized Grade II-III teeth mobility
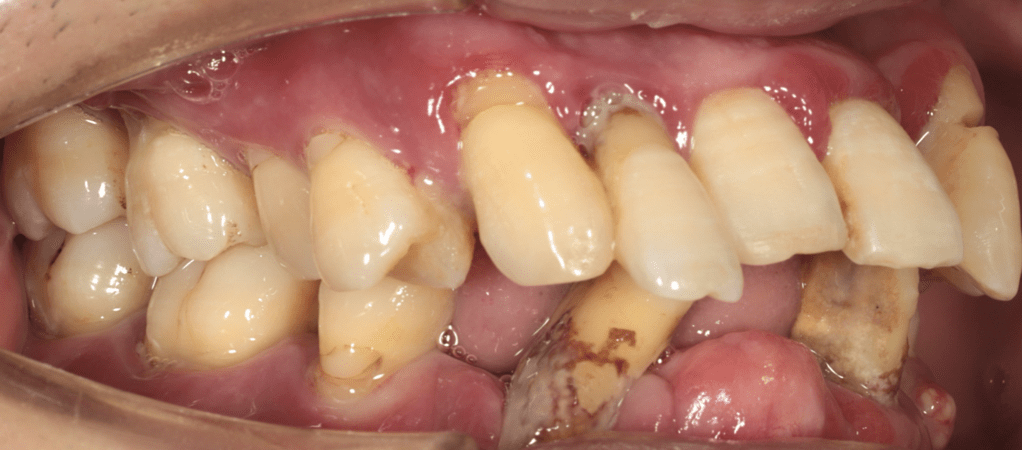
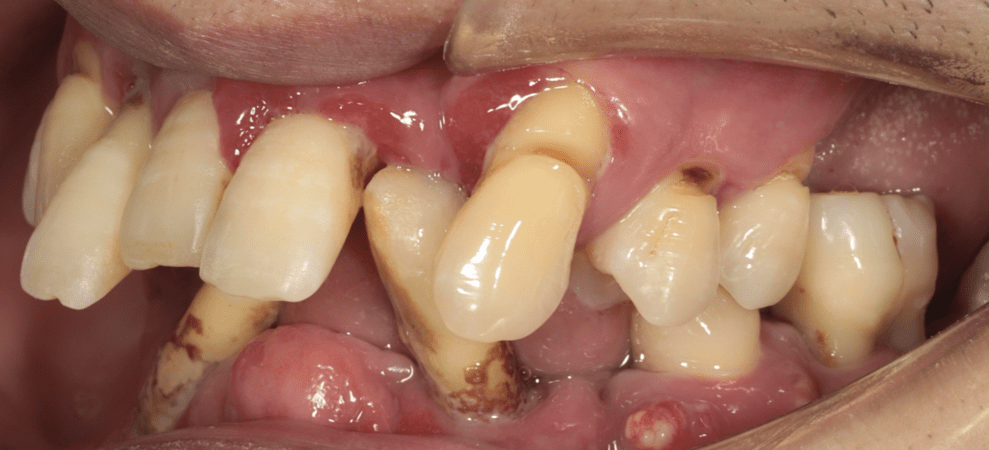

Extensive bone loss and periapical pathology
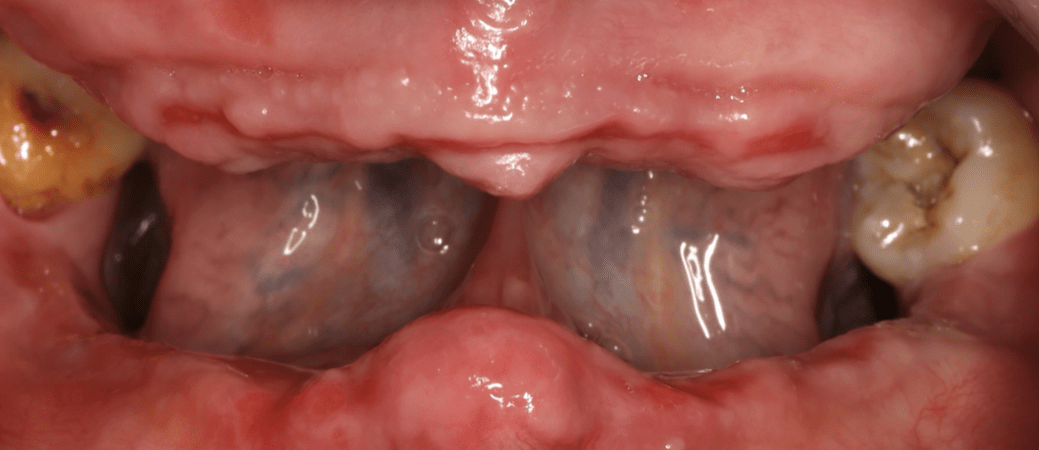
Tooth extraction and tissue healing


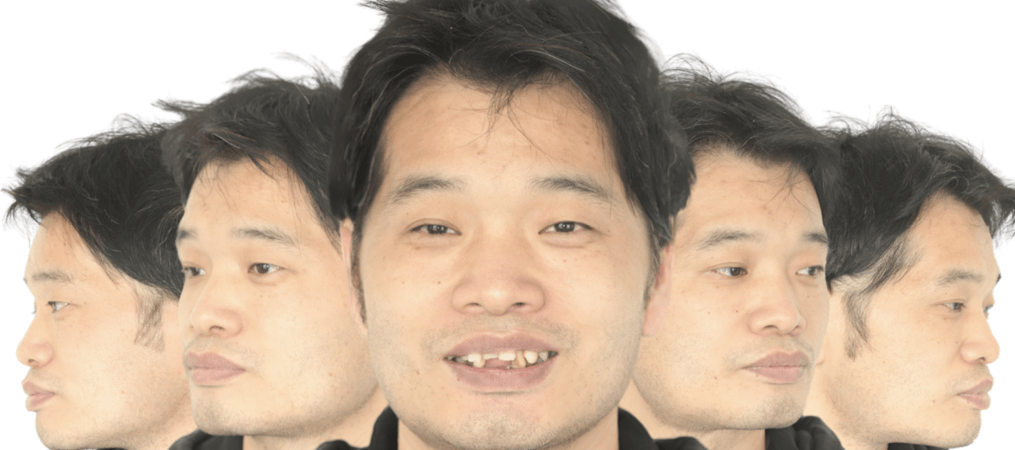
Significant enhancement in facial esthetics following denture delivery
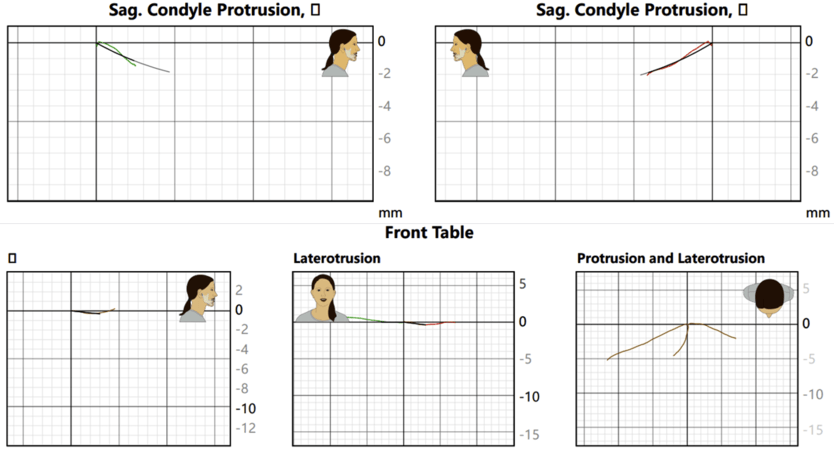
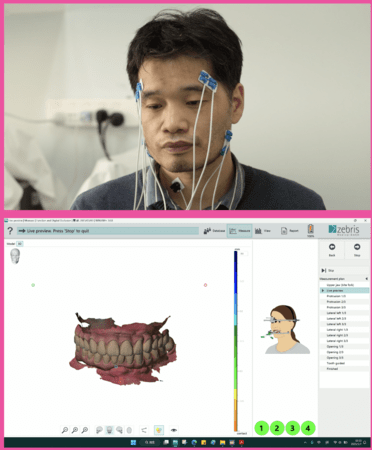
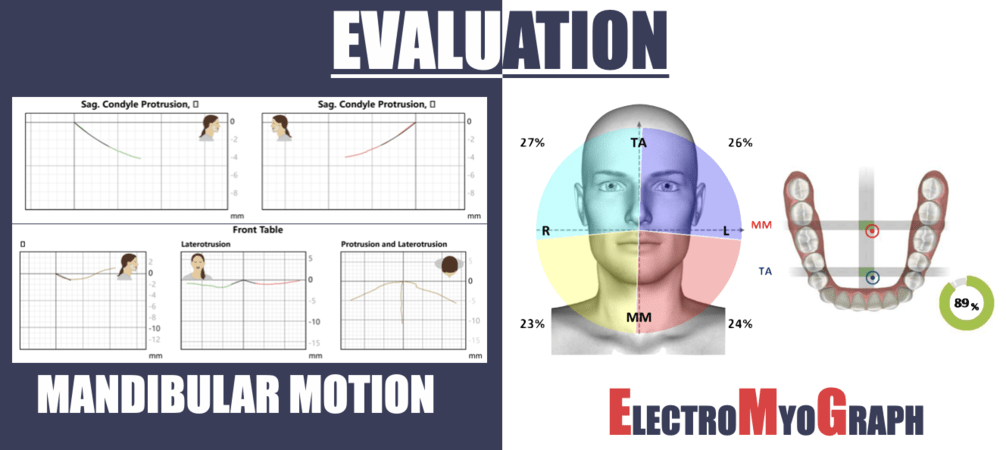
Verified coordinated activity of the masticatory muscles and TMJ during function with the interim.
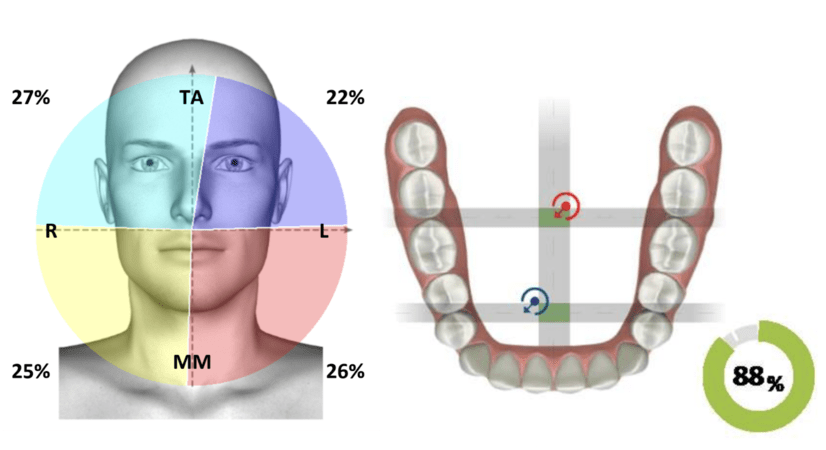
verified coordinated activity of the masticatory muscles and TMJ during function with the interim.
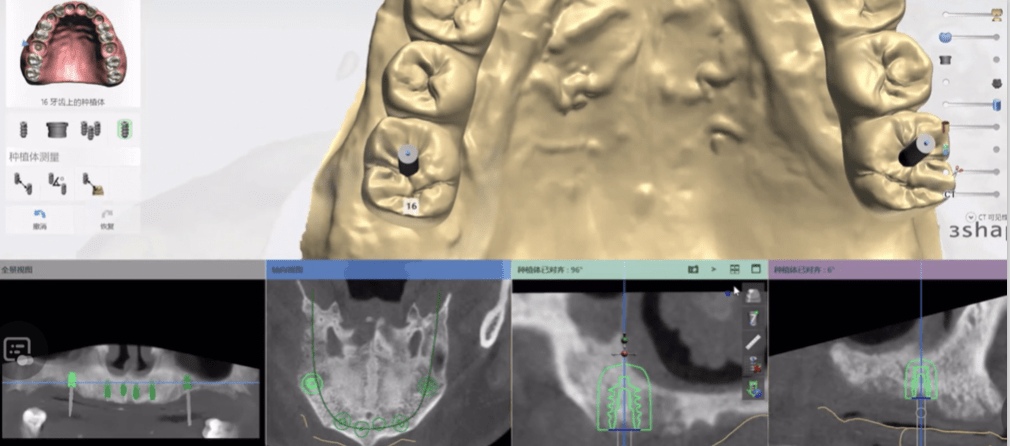
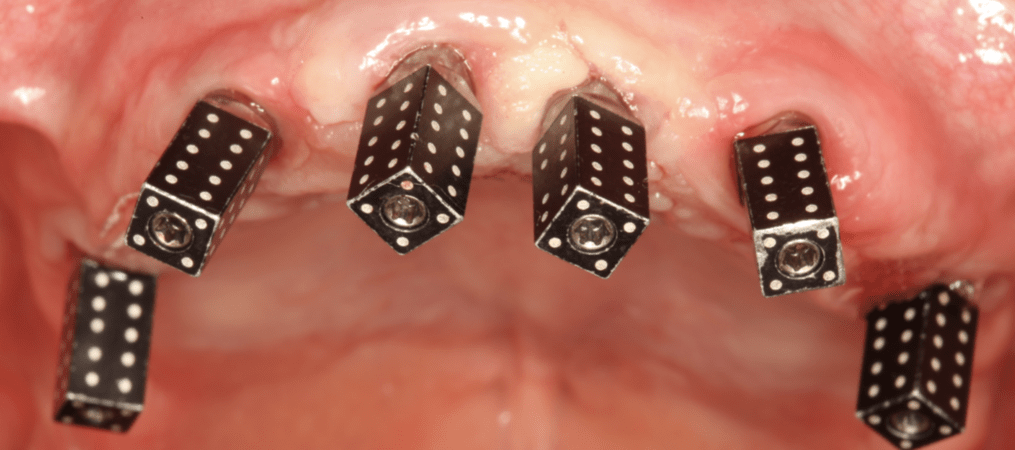
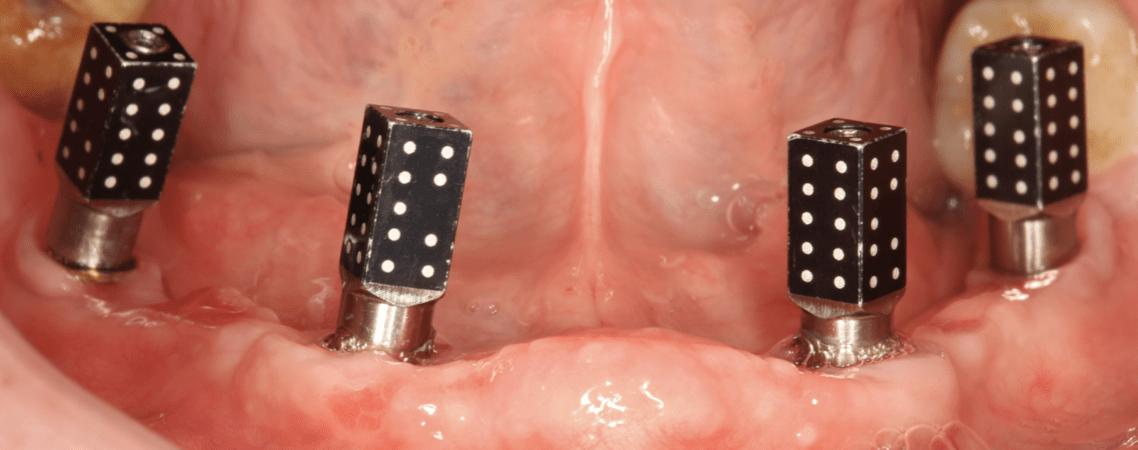
To achieve optimal implant positioning and immediate loading.
Progress & Completion


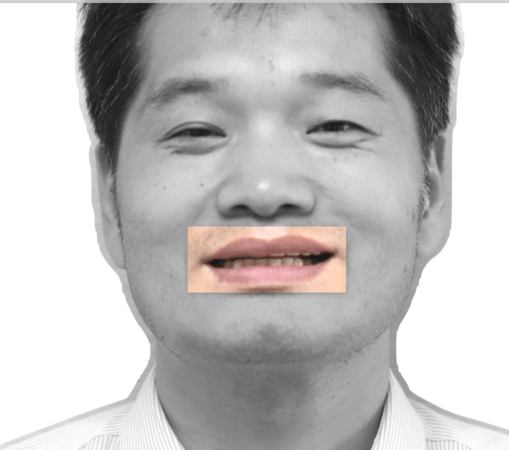
Also indicating insufficient anterior teeth exposure


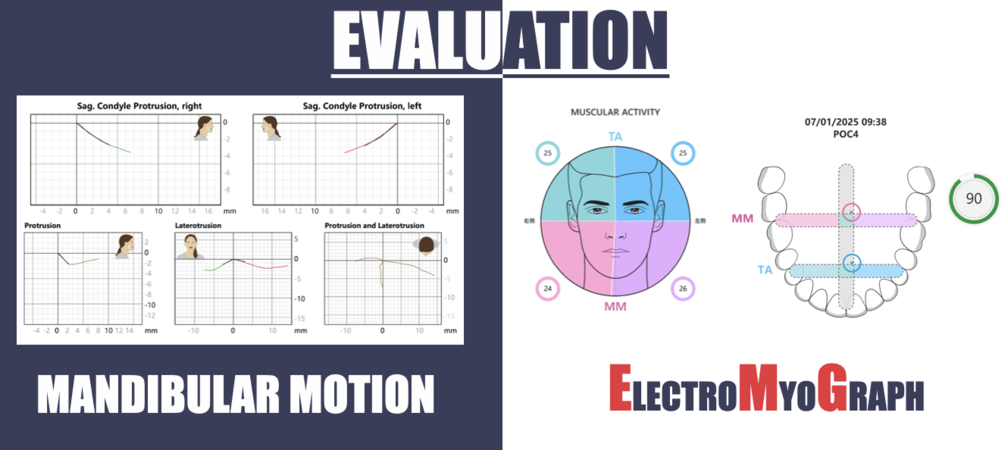
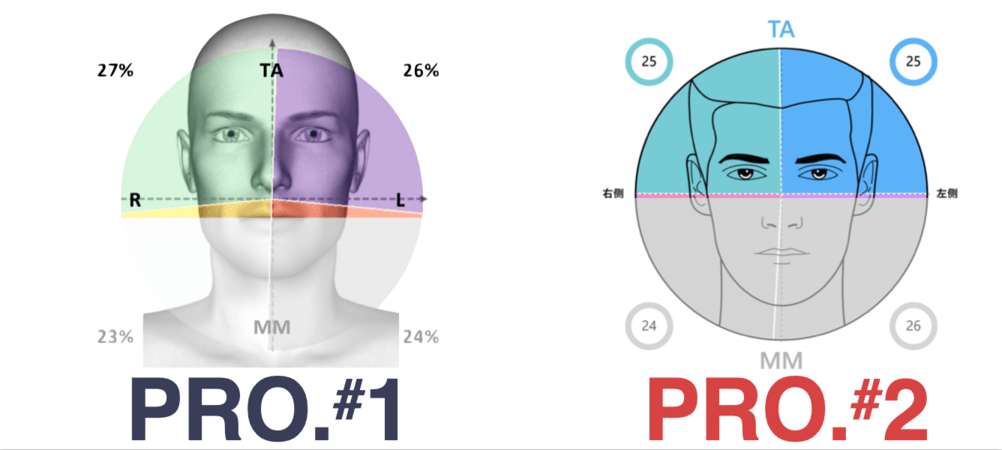
Electromyographic assessment confirmed better functioning of the 2nd provisional restoration.
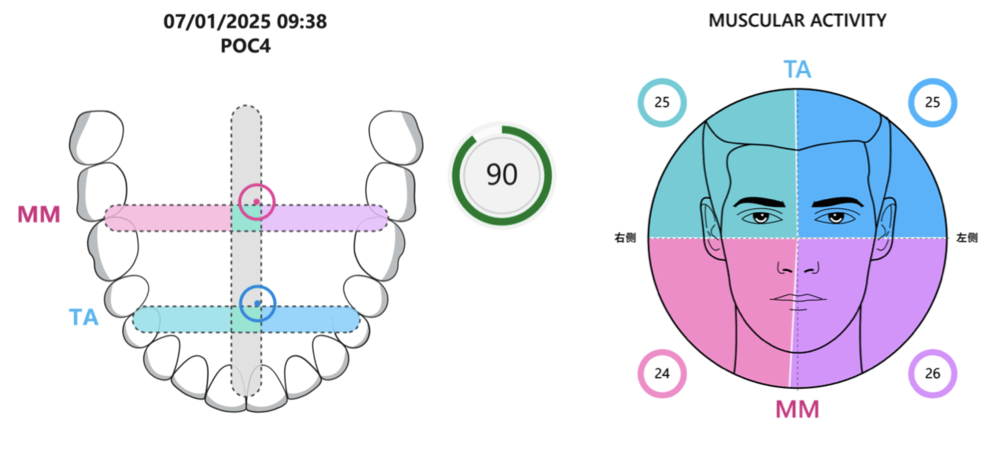
between the temporalis and masseter muscles.
Profiles from the first and second provisionals confirmed the successful establishment of an appropriate VDO.

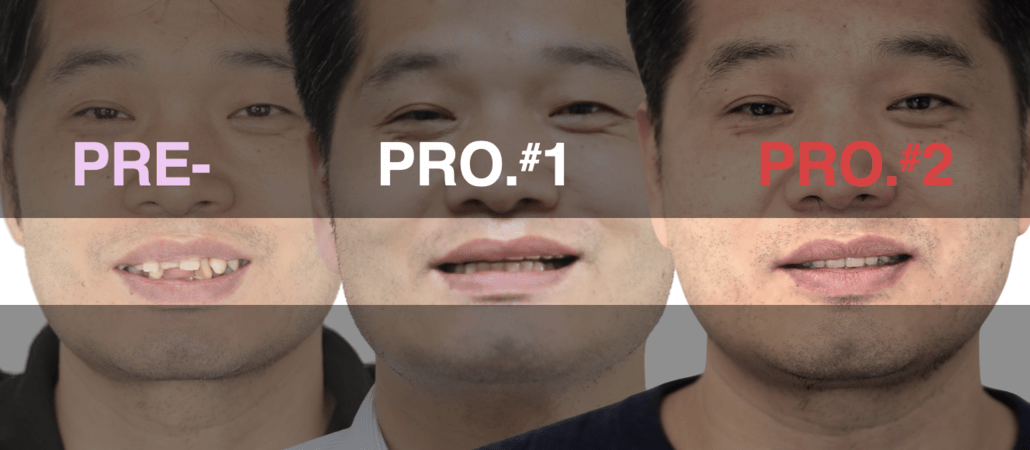
This correction created a more natural lip-tooth relationship and significantly enhanced smile line.
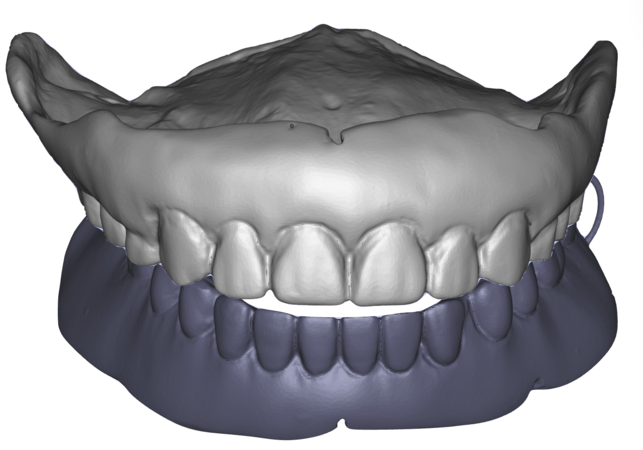
The treatment began with full-mouth extraction due to the extensive infection and poor prognosis of the existing dentition. An interim removable denture was delivered to establish a baseline vertical dimension of occlusion and provide immediate functional and aesthetic rehabilitation.
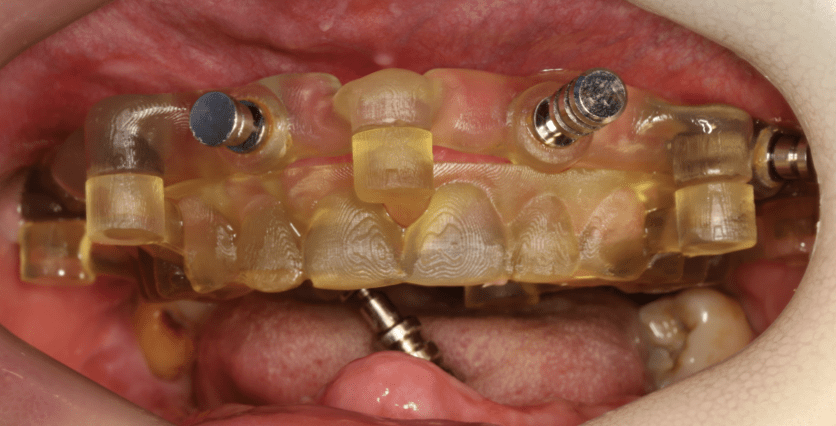
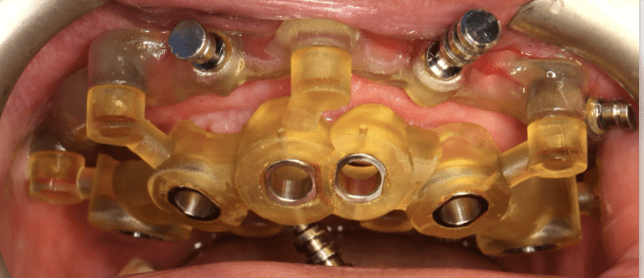
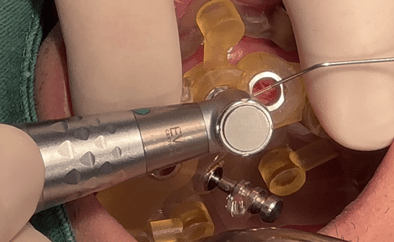
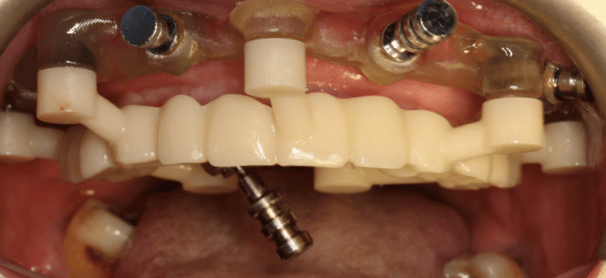
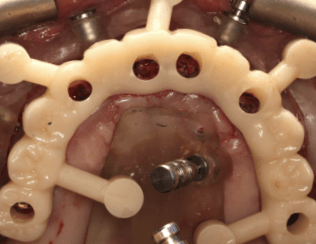
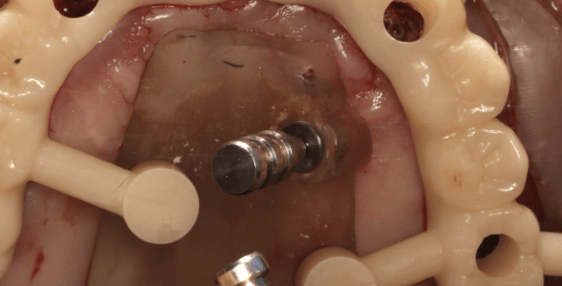
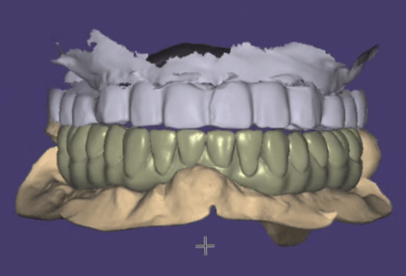
Following a healing period, implant placement was performed using a digitally guided approach. The use of stackable guides and a virtual patient workflow allowed for highly accurate implant positioning, ensuring alignment with the planned prosthetic outcome and optimizing biomechanical distribution.
A staged prosthetic protocol was implemented, including first and second provisional restorations. These provisional phases were critical to progressively increase the vertical dimension of occlusion, allowing neuromuscular adaptation and functional validation through repeated clinical and electromyographic evaluations.
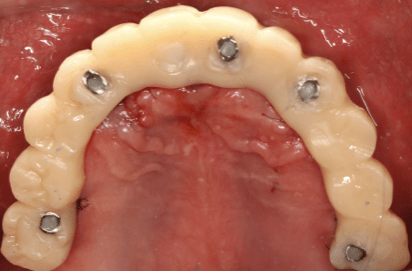
After achieving functional stability and patient adaptation, the definitive implant-supported full-arch restorations were delivered. The final prostheses restored occlusion, aesthetics, and function, completing the full-mouth rehabilitation in a controlled and predictable manner.
Follow-up & Outcome


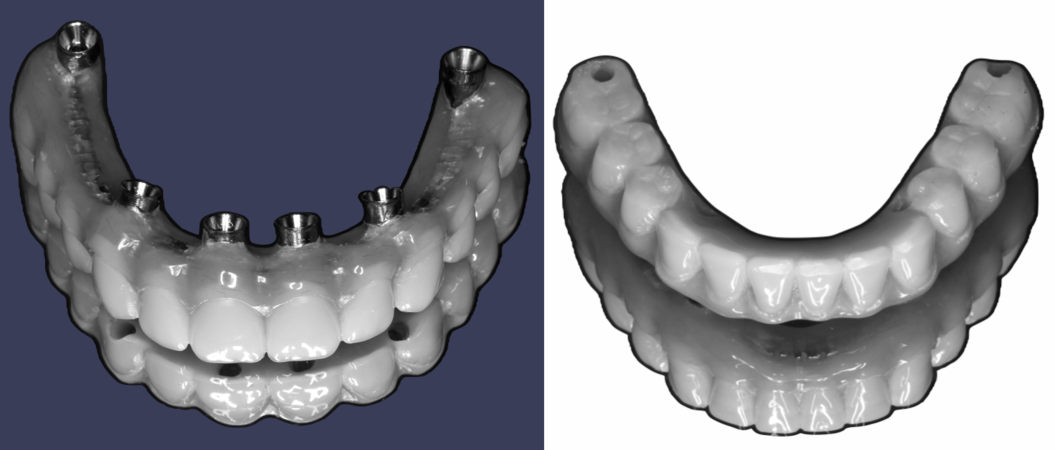
Which meticulously replicating the design of the second provisional.

Final restoration



Long-term stability of the patient’s facial and dental aesthetics after full-mouth rehabilitation.


OPG confirms stable and accurate seating of the final restorations, with maintained marginal bone level

Post-treatment follow-up demonstrated favorable clinical outcomes, with stable implant integration and healthy peri-implant tissues. The patient showed no signs of inflammation or complications, indicating successful resolution of the initial infectious condition.
At the one-year follow-up, the prosthetic restorations remained stable, with no mechanical or biological complications observed. The occlusion was well maintained, and the increased vertical dimension of occlusion proved to be functionally and aesthetically sustainable over time.
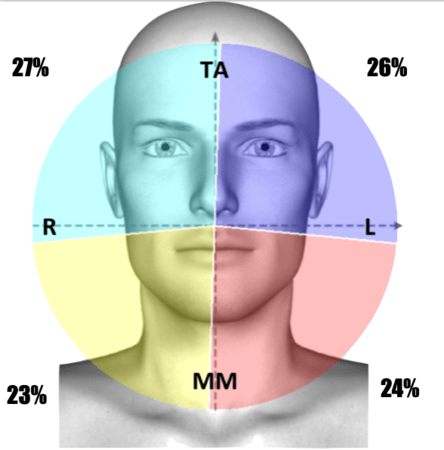
Functional assessments confirmed improved muscle coordination and efficiency, as evidenced by electromyographic analysis. The staged approach to VDO reconstruction contributed significantly to the patient’s neuromuscular adaptation and long-term comfort.
From an aesthetic and patient-centered perspective, the outcome was highly satisfactory. The rehabilitation restored facial proportions, smile aesthetics, and masticatory function, significantly improving the patient’s quality of life and demonstrating the effectiveness of a digitally planned, staged full-mouth rehabilitation approach.
Questions
Ask a question
Lado esquerdo da prótese.
Em relação ao último implante do lado esquerdo do paciente. A região mostra contato da estrutura da prótese com osso, verticalmente. Esta situação não causaria inflamação. ?
Em relação ao último implante do lado esquerdo do paciente. A região mostra contato da estrutura da prótese com osso, verticalmente. Esta situação não causaria inflamação. ?

Throughout the 1-year follow-up period, there have been no clinical signs of inflammation, discomfort, or peri-implant pathology in that region. The definitive prosthesis is stable and the surrounding soft tissue remains healthy.
The "vertical contact" observed in the imagery is largely an artifact of the projection angle typical of panoramic radiographs. Because a 2D image collapses three-dimensional structures, it often creates a visual superimposition (overlap) of the prosthetic framework and the bone. Clinical examination confirms adequate clearance, and we will continue to monitor the site during routine maintenance.
Why would you leave the lower wisdom teeth?
In reply to Why would you leave the lower wisdom teeth? by Anonymous
Initially, the lower wisdom teeth were preserved to serve a functional purpose during the transition phase: they provided stability for the interim complete denture and assist in the positioning of the surgical guide system.
While our clinical recommendation was to extract both teeth to simplify the long-term prosthetic environment, the patient expressed a strong personal desire to keep his remaining natural teeth. After a detailed discussion regarding potential risks and future complications, we respected the patient's autonomy. At the 1-year follow-up, the clinical status of both wisdom teeth remained stable, with no signs of pathology.