Full-Mouth Rehabilitation Using Vertical Preparation Technique
A 69-year-old female patient presented to the clinic seeking improvement in both the appearance and function of her dentition. Her chief concerns included compromised esthetics, difficulty during mastication, and generalized discomfort associated with dentin hypersensitivity. The patient expressed a clear desire for a comprehensive oral rehabilitation that would restore function, improve occlusal stability, and deliver a natural and harmonious smile. Given the complexity of the case, a fully digital and biologically guided approach was selected to ensure predictability, precision, and long-term stability.
Evaluation & Diagnosis


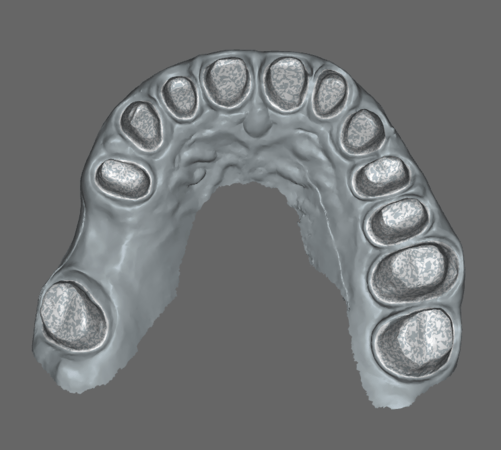
Preoperative clinical view of upper maxilla

Frontal view with the central incisor fractured.
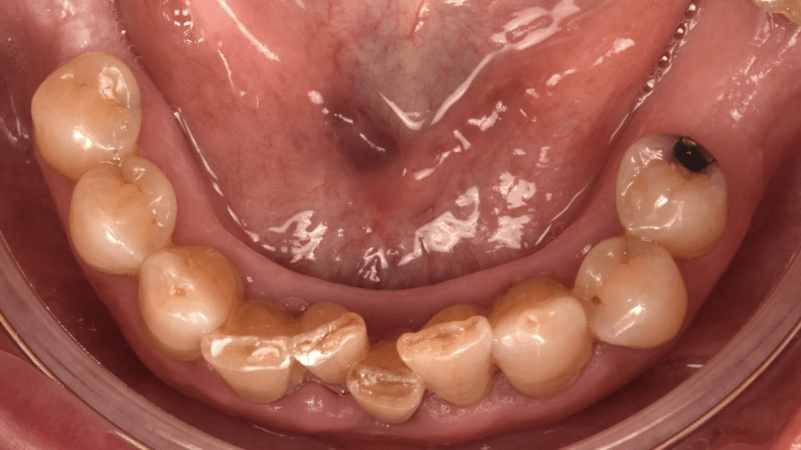


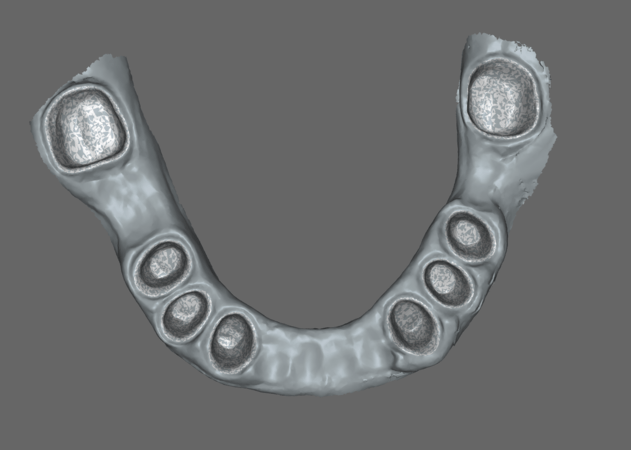
Clinical examination revealed malpositioned teeth, partial edentulism affecting the premolar and molar regions, generalized tooth discoloration, and signs of dentin hypersensitivity. The occlusal relationships were altered, and the smile line lacked harmony due to both tooth position and tissue irregularities. A comprehensive digital diagnostic protocol was implemented, including intraoral scanning, radiographic analysis, and cone beam computed tomography (CBCT). These records were digitally integrated to evaluate bone anatomy, remaining tooth structure, and occlusal dynamics.
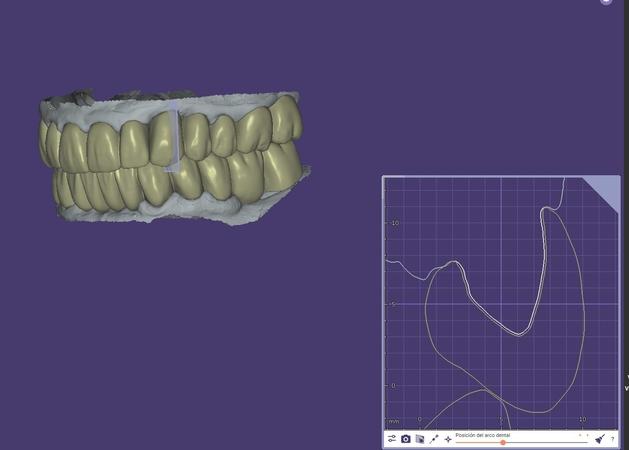
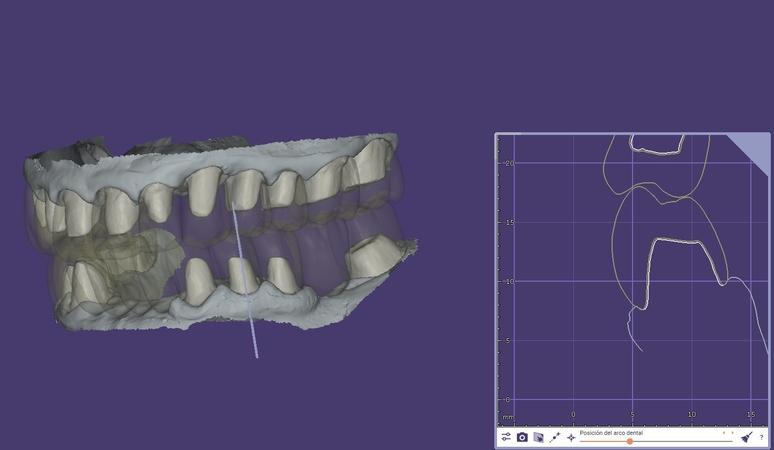
A digital wax-up was created using a fully digital workflow with 3Shape® software, allowing visualization and validation of the proposed restorative outcome. This step was fundamental for assessing esthetic parameters, occlusal vertical dimension, and functional guidance prior to any irreversible procedures. Based on the diagnostic findings, a full-mouth rehabilitation was planned. The Biologically Oriented Preparation Technique (BOPT) was selected as the core restorative concept to guide soft tissue conditioning and emergence profile development on natural teeth.
Progress & Completion
Biologically Oriented Preparation Technique (BOPT) of the upper arch
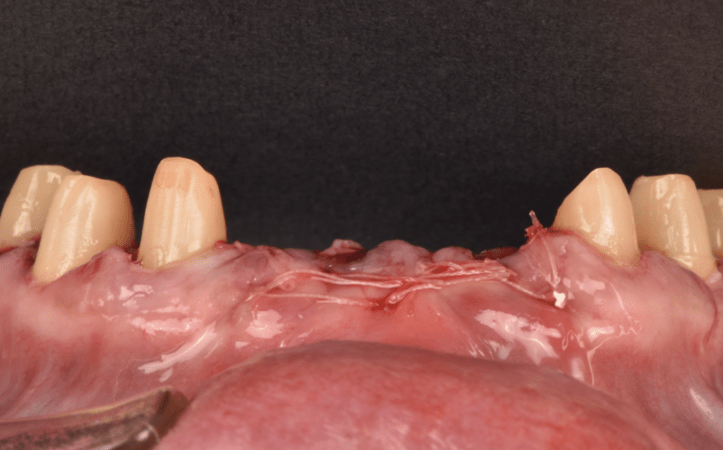
Extraction of the central and lateral incisors
The fitting of the impression coping using the periapical radiograph was analyzed.

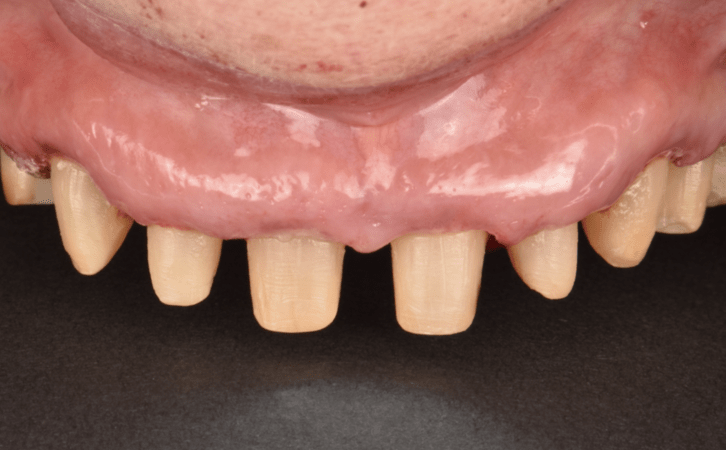
Polymethyl methacrylate (PMMA) provisional crowns on natural dentition

PMMA crowns on natural dentition

Provisional restoration.

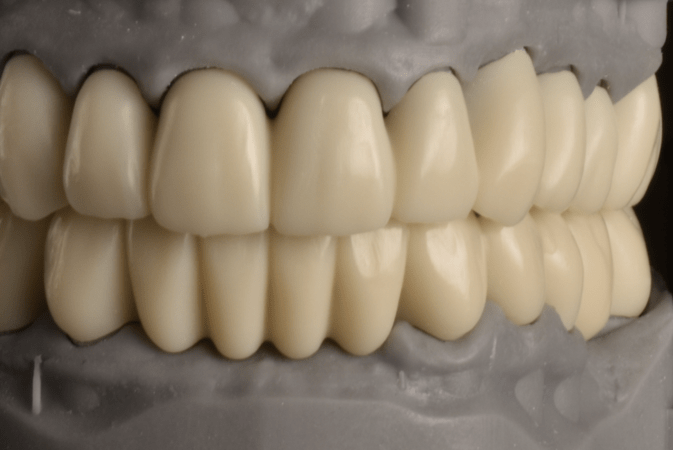
Resin prototype try-in for evaluation of esthetic and functional parameters prior to zirconia fabrication

Frontal view of the prototype try-in

Upper arch BOPT preparation and periodontal healing


Evaluation of the position, shape and occlusal movements.

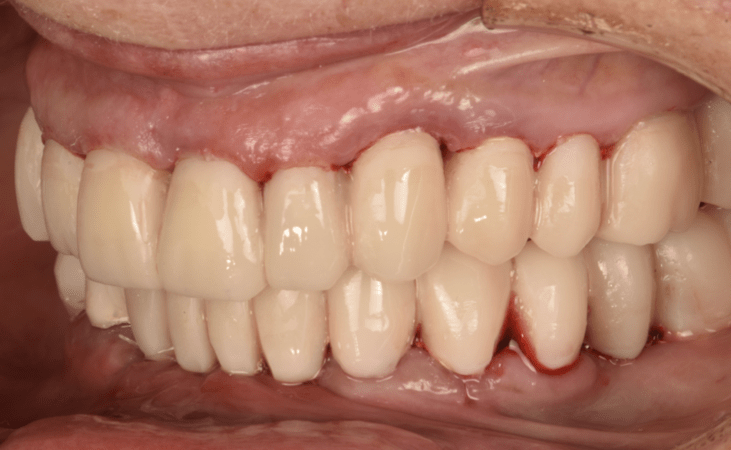
Final restoration
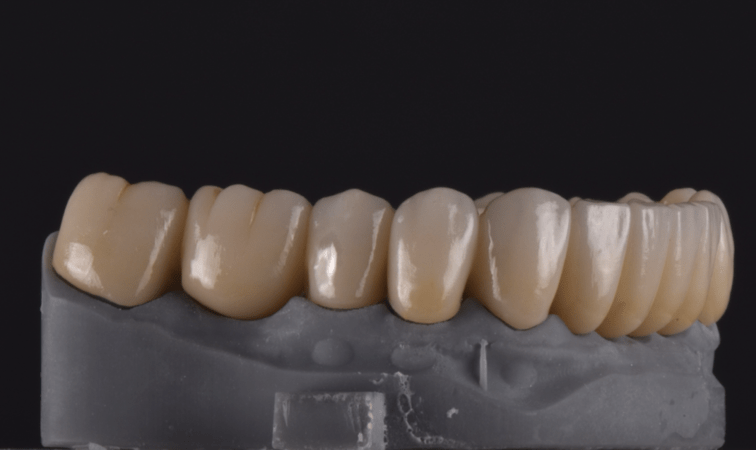
Full arch monolithic zirconia crowns
The treatment phase began with biologically driven tooth preparations following the BOPT protocol. This approach allowed the prosthetic contours to guide gingival adaptation without a predefined finish line, promoting stable and healthy soft tissue architecture.
The management of VDO was established using a Lucia jig, allowing determination and maintenance of the correct vertical dimension at the appropriate mandibular position prior to the provisional restorations. Provisional restorations played a crucial role in the treatment sequence. They were fabricated based on the digital wax-up and used to refine occlusion, phonetics, esthetics, and gingival contours. Crown lengthening was not required in this case, as the BOPT technique allowed for adequate emergence profiles and prosthetic margins without the need for surgical crown lengthening.
The provisional crowns were cemented using Kerr TempBond™ Clear, providing reliable retention while allowing easy retrievability during the evaluation and tissue maturation phase. Throughout this stage, occlusal adjustments and soft tissue conditioning were carefully monitored to achieve optimal functional and biological integration.
Once stability and patient satisfaction were confirmed, the definitive restorations were fabricated in zirconia. Monolithic zirconia was selected for posterior regions to ensure strength and durability, while layered zirconia was used in the anterior zone to enhance esthetics. The restorations were segmented rather than splinted as a single unit. They were divided into three sections in both the maxillary and mandibular arches: from molar to first premolar, from canine to canine, and from first premolar to molar.
All final restorations were cemented using Kerr Maxcem Elite™ Chroma, a self-adhesive resin cement that offers high bond strength, excellent marginal sealing, and chromatic control during cementation. In addition, Kerr OptiBond™ Universal was incorporated where indicated to enhance adhesion on prepared tooth surfaces, reinforcing the long-term stability of the restorations.
Follow-up & Outcome

Final outcome of the fixed partial denture on central and lateral incisor.

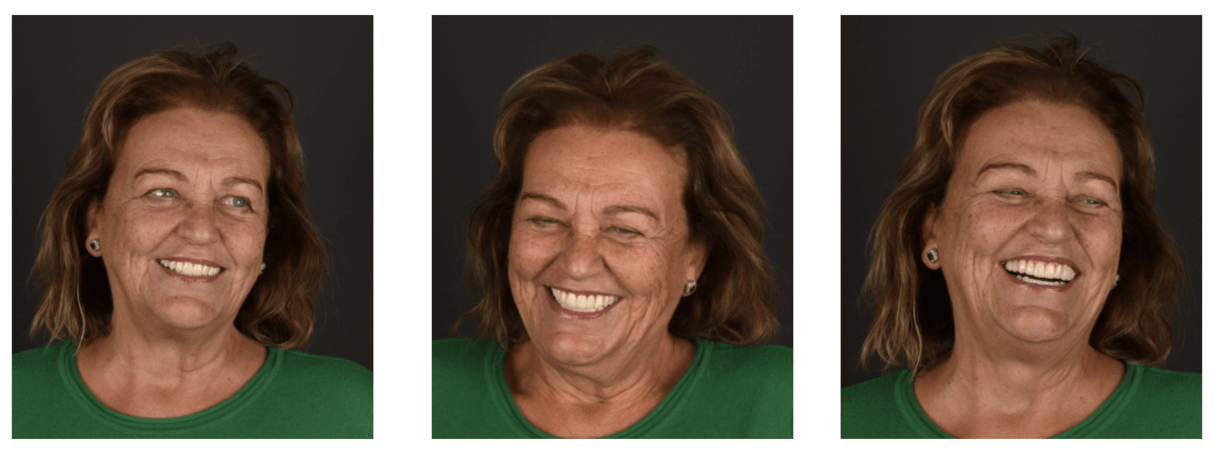
Frontal view of the smile. Look into the harmony and symmetry of the central and lateral incisors.

Frontal view of the final restoration
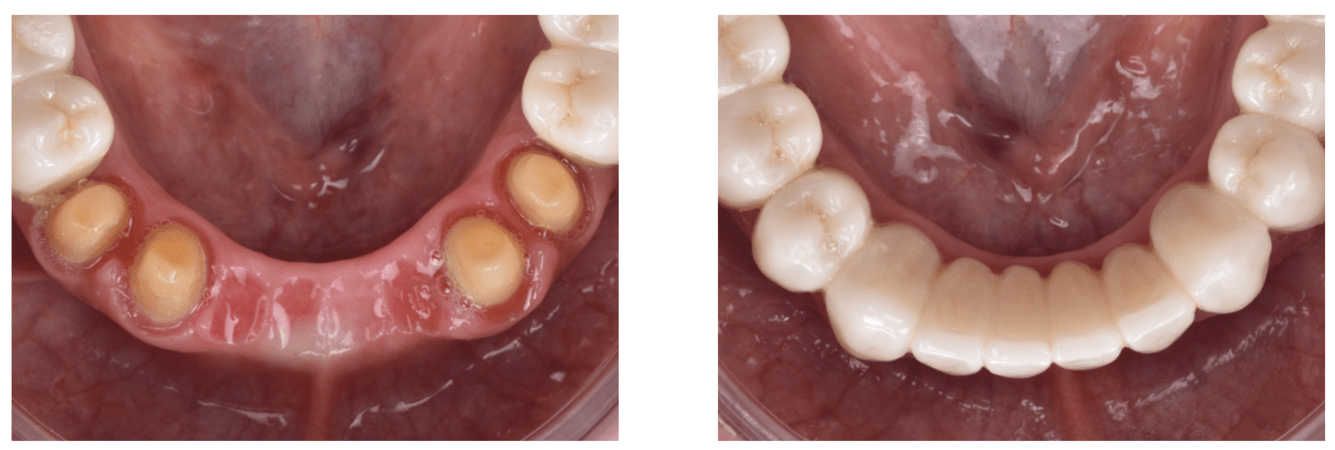
Intraoral view of the anterior area of the final restoration.

The patient was followed clinically for a period of three years, during which excellent biological, functional, and esthetic stability was observed. No postoperative sensitivity, inflammation, or prosthetic complications were reported. The soft tissues adapted harmoniously to the prosthetic emergence profiles, demonstrating the effectiveness of the BOPT approach.
Occlusal stability and masticatory efficiency remained consistent over time, and the color integration of the zirconia restorations continued to be highly satisfactory.
The patient reported a significant improvement in comfort, confidence, and overall quality of life. This case confirms the clinical reliability of combining a fully digital workflow with biologically oriented prosthetic concepts and high-performance restorative materials. The integration of Kerr products throughout the provisional and definitive phases contributed to a predictable, efficient, and patient-centered rehabilitation with long-term success.
Hygiene therapy and maintenance protocol
Prior to the definitive prosthetic phase, the patient underwent comprehensive hygiene therapy, including professional supragingival and subgingival cleaning and individualized oral hygiene instructions. After completion of the full-mouth rehabilitation, the patient was enrolled in a strict maintenance and recall program, consisting of periodic professional hygiene sessions and clinical evaluations at regular intervals. This protocol was aimed at ensuring periodontal stability, preserving peri-prosthetic tissue health, and promoting the long-term success of the restorations.
This case demonstrates the clinical reliability of combining digital workflows with the BOPT approach for comprehensive oral rehabilitation. The integration of prosthetic and surgical planning allows predictable soft tissue management and esthetic enhancement.
Utilizing BOPT crowns provides continuity in the emergence profile and ensures long-term biological and mechanical stability. The patient-centered, digitally guided process resulted in a highly functional and esthetically pleasing outcome with excellent tissue health and patient satisfaction.
Additional resources


Questions
Ask a question
How was dentin hypersensitivity managed?
How was it possible to prepare crowns without aggravating pre-existing hypersensitivity? How could you conquer hypersensitivity without root canal treatment?
How was it possible to prepare crowns without aggravating pre-existing hypersensitivity? How could you conquer hypersensitivity without root canal treatment?

Dear Sandeep Sherma, thank you for your questions.
Hypersensitivity was managed conservatively. After tooth preparation, we performed Immediate Dentin Sealing (IDS) using OptiBond™ Universal (Kerr). This allowed us to seal the freshly cut dentin, reduce fluid movement, and minimize postoperative sensitivity. Proper provisionalization with good marginal adaptation was also essential to protect the pulp during the interim phase.
The preparations were carried out with careful technique, adequate water cooling, and controlled reduction. Immediately sealing the dentin with OptiBond Universal helped prevent bacterial penetration and reduced the risk of increasing sensitivity. This approach is well supported in the literature as an effective way to reduce postoperative discomfort.
Current literature clearly indicates that it is not necessary to perform endodontic treatment routinely before crown preparation in vital teeth, provided there are no signs of irreversible pulpitis. With correct diagnosis, minimally traumatic preparation, and proper dentin sealing, hypersensitivity can be controlled while maintaining pulp vitality.
Thank you again for your interest in the case.




Where is the smile line? Did the posterior bridges have a long spam?
Which prosthetic material was used to address this factor?Did the patient present any bruxism due to the weak posterior occlusion?Thank you for sharing your experience.
Which prosthetic material was used to address this factor?
Did the patient present any bruxism due to the weak posterior occlusion?
Thank you for sharing your experience.
In reply to Where is the smile line? Did the posterior bridges have a long spam? by Nabih Joseph Badawi
Dear Nabih Joseph Badawi,
The smile line was clinically evaluated during the esthetic analysis phase. The patient presented a medium smile line, which allowed us to manage the anterior restorations with controlled gingival exposure and proper integration with the upper lip dynamics.
Second, the posterior bridges involved spans due to the missing teeth. This was carefully planned to reestablish posterior support and recover a stable occlusal scheme.
Next question, regarding the material, monolithic zirconia was selected for the posterior bridges. This material was chosen because of its high mechanical resistance and reliability in long-span situations under significant occlusal load.
And the last question: no parafunctional problems were recorded. As part of the maintenance protocol, the patient was provided with a maxillary Michigan-type occlusal splint for protection and long-term stability.
Thank you for your interest in the case!