Digital & biological approach in full arch rehabilitation
The patient is a 51-year-old systemically healthy woman presenting with multiple chief complaints: significant esthetic concerns, a pronounced gummy smile, and occlusal dysfunction. Clinical and facial photographs confirmed a high smile line with excessive gingival display, while the intraoral examination revealed a severely compromised dentition with existing restorations, missing teeth, and an irregular alveolar crest consistent with Cawood & Howell Class III–IV bone resorption patterns. The panoramic radiograph showed residual teeth with poor long-term prognosis in both arches, along with evidence of alveolar ridge irregularities and vertical bone loss in the transition zone.
The diagnostic challenge was framed as a fundamental decision between a tissue reduction approach (alveoloplasty) versus a biologically conservative regenerative strategy to address the gummy smile and manage the transition zone. Considering the patient's esthetic demands, high smile line, and available bone volume, the team opted for a full-arch implant rehabilitation under the FP-1 concept — a fixed, tissue-supported prosthetic category — integrating a biological and digital workflow within a Perio-Prostho interdisciplinary approach.
Evaluation & Diagnosis


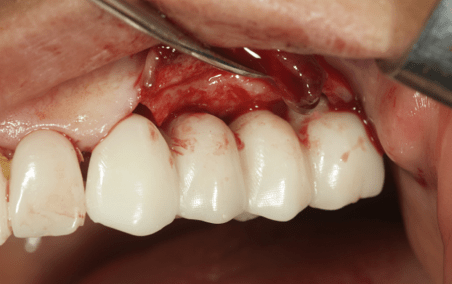
Transition zone, rigid temporary prosthesis, alveolar crest irregularities.

Gummy smile
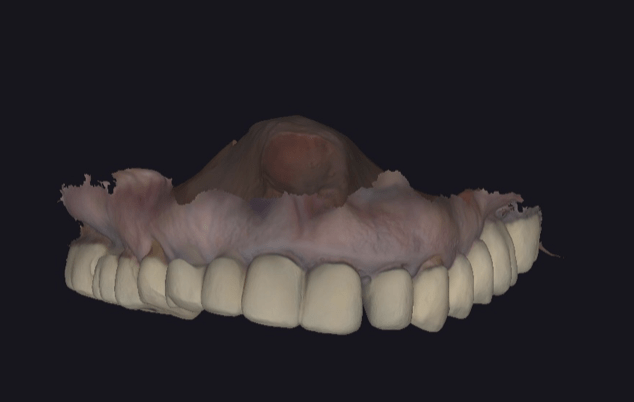
Baseline
Progress & Completion
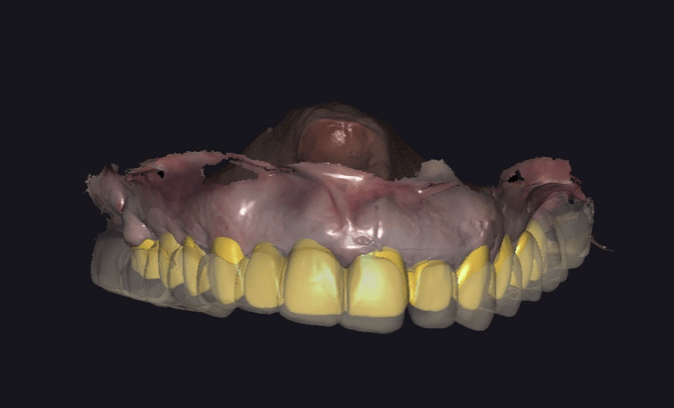
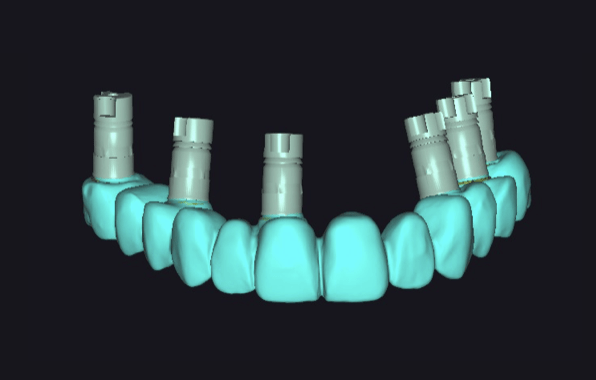
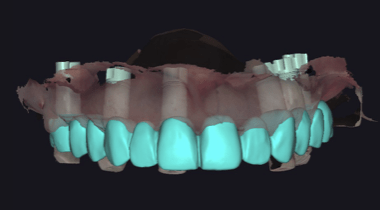
Digital design

Gallucci Prosthesis
Execution
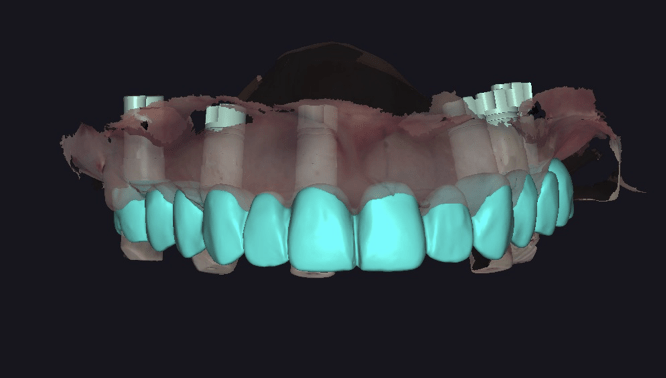
Matching
Production

Baseline

Digital design

Matching

Pontic design

Pontic design
Matching

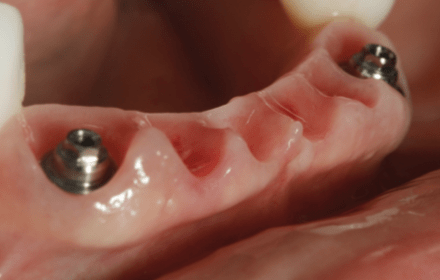
Guided Soft Tissue Healing
Guided Soft Tissue Healing
Biological Pontic Heigh (maxilla 2,32 mm)

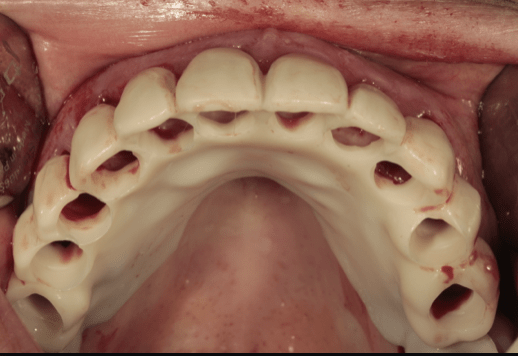
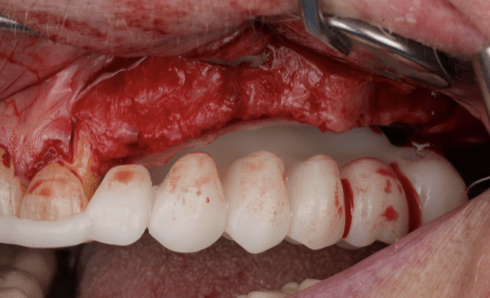
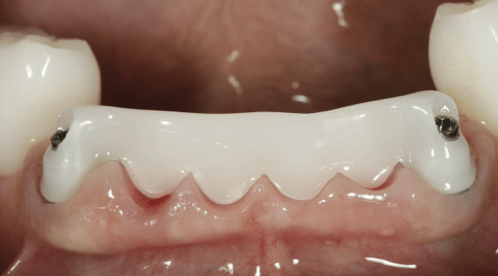
Temporary prosthesis
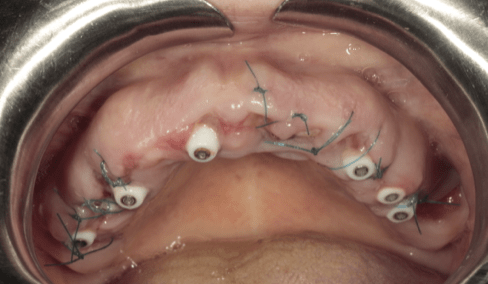
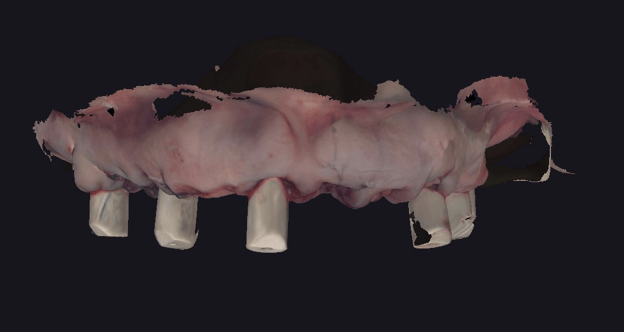
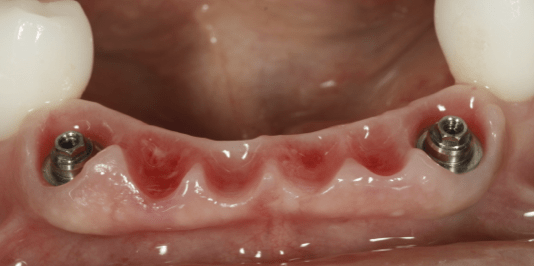
Implant placement & Healing caps

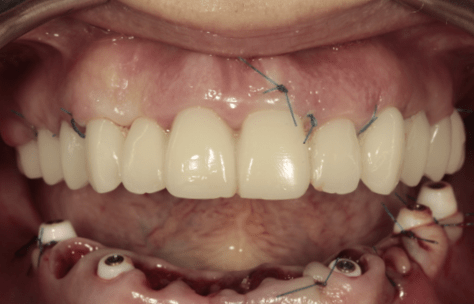
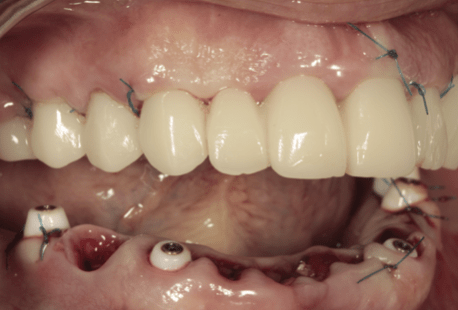

Temporary prosthesis



Healing phase

Healing phase


Temporary prosthesis

Upper arch
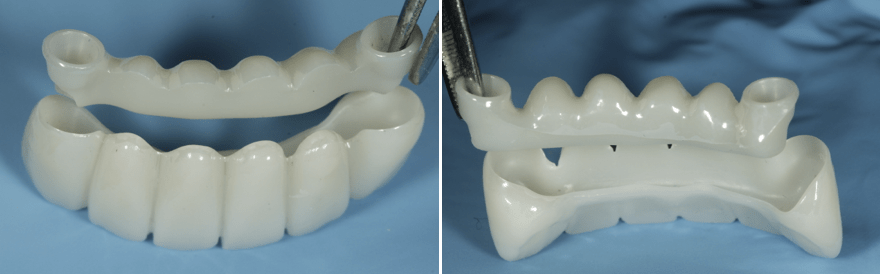
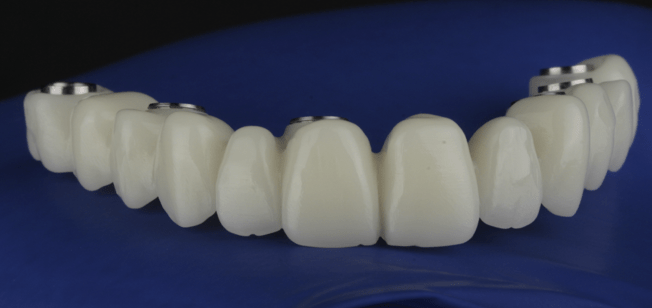
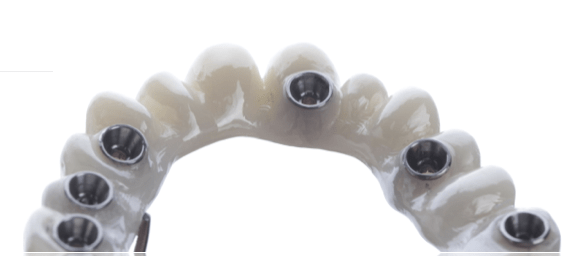
Zirconia prosthesis
Treatment was structured around a six-step digital protocol: (1) Baseline data acquisition, (2) Digital smile design, (3) Prosthetic planning following the Gallucci protocol, (4) Surgical execution, (5) Digital matching of pre- and post-operative data, and (6) CAD/CAM production of restorations.
Surgical execution involved full-arch implant placement in both maxilla and mandible. Immediately following surgery, an intraoral scan (IOS) was performed to capture post-operative tissue anatomy, which was then merged with pre-operative design data to guide the fabrication of the immediate-load provisional prosthesis, printed in SprintRay OnX Tough2 material (a high-performance PMMA-based resin).
Temporary prosthesis and soft tissue management constituted the most biologically nuanced phase. Guided soft tissue healing was achieved through strategic pontic design, referencing Pozzi et al. (2014). The biological pontic height measured 2.32 mm in the maxilla and 2.20 mm in the mandible (average 2.26 mm), providing sufficient vertical space for tissue maturation without aggressive compression. Pontic design selection followed the Gomez-Meda & Esquivel (2022) classification: a flat pontic was chosen in areas with ideal vertical tissue volume (Seibert Class I), a step pontic where ridge defects were under 1 mm (Class II), and an ovate pontic where mild defects under 2 mm existed (Class III). The goal was maximized tissue contact without pressure, allowing natural architecture to develop over the healing period.
Clinical photographs during the provisional phase showed progressive soft tissue adaptation, with well-defined emergence profiles and healthy gingival margins around implant abutments. Intraoral views at the 4th month confirmed stable peri-implant tissue height and contour maturation.
Final prosthesis fabrication was guided by the tissue-conditioned emergence profile transferred from the temporaries. Referencing Linkevicius (2017), zirconia was selected as the material of choice for its biocompatibility with soft peri-implant tissues. The definitive restorations were designed as screw-retained, monolithic full-arch zirconia bridges for both arches. The intaglio surfaces were designed to replicate the emergence profile established by the provisionals, ensuring a seamless biological transition. The comparison between temporaries, the monolithic zirconia framework, and the final polished prosthesis demonstrated excellent morphological transfer throughout the workflow.
Follow-up & Outcome





Delivery

Delivery

1st year

2nd year

3rd year

Intial - Temporary prosthesis - Zirconia prosthesis - Follow-up 40th month.
The patient was followed at delivery, 1st year, 2nd year, 3rd year, and up to the 40th month post-delivery. Intraoral photographs at each interval consistently demonstrated stable peri-implant soft tissue levels with no signs of recession, inflammation, or tissue collapse under the pontics. The gingival architecture maintained the contours originally shaped by the temporary prosthesis throughout the entire follow-up period.
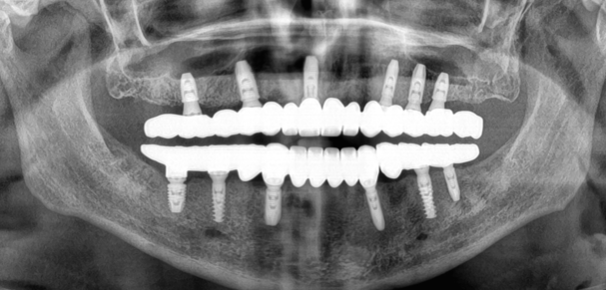
From a radiographic standpoint, the panoramic X-ray at 2 years showed all implants well-integrated with no visible marginal bone loss, and the digital superimposition of post-operative and 4th-month IOS scans confirmed dimensional tissue stability. The soft tissue volume analysis illustrated consistent ridge preservation without the need for any regenerative or corrective intervention during follow-up.
Facially, the four-phase portrait comparison (Initial → Temps → Zirconia → 40th month) was visually striking: the patient's gummy smile was fully resolved, the lip-tooth relationship was harmonious, and the final smile was natural, proportionate, and face-driven — achieving the esthetic objectives defined at baseline without any tissue grafting or surgical reduction.
The case concluded with four key takeaways: the high smile line was successfully managed through prosthetic means alone; the treatment was biological, conservative, and face-driven; the FP-1 prosthetic design acted as a natural prosthetic barrier protecting the peri-implant tissues; and the emergence profile architecture made the final restoration easy to clean and maintain long-term.
Hi there, i am in awe of the transformational work carried out here its truly life changing/giving and i salute all of you