Management of an iatrogenic case following traumatic tooth extraction, bone graft and implant failure
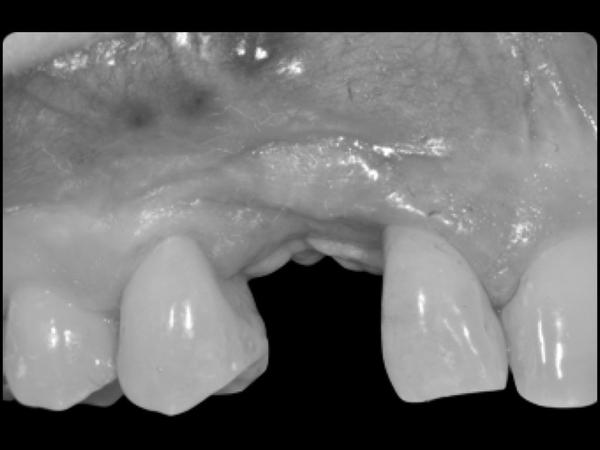
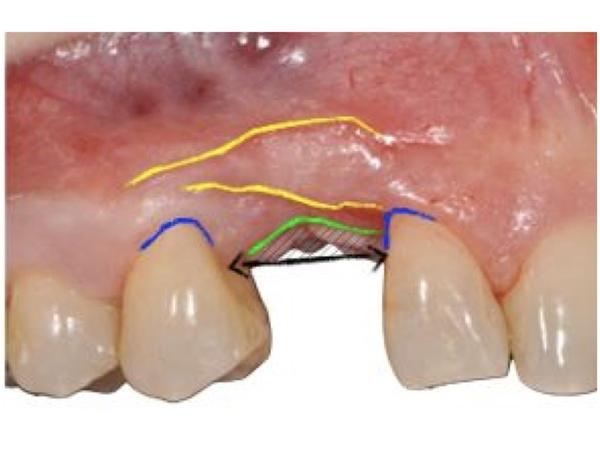
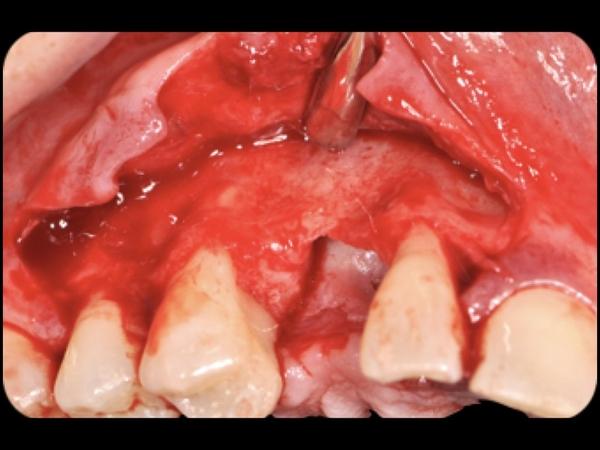
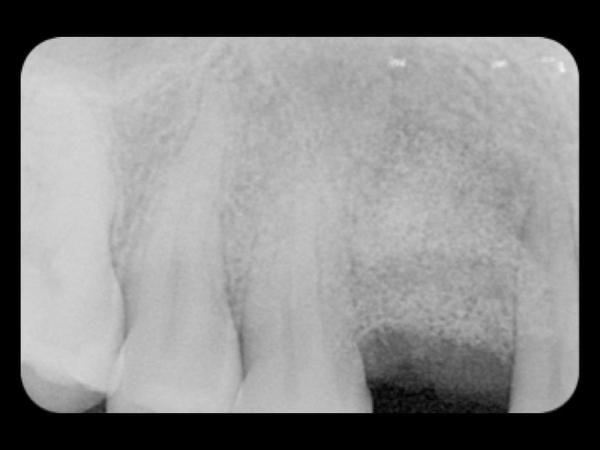
A 30-year-old female patient who lost tooth #13 FDI (#6 US). She reported the traumatic extraction of the canine, which resulted in a significant vertical bone loss of 3 mm and an advanced horizontal lingual defect. After the extraction, a bone graft and an implant insertion were attempted: both graft and implant failed.
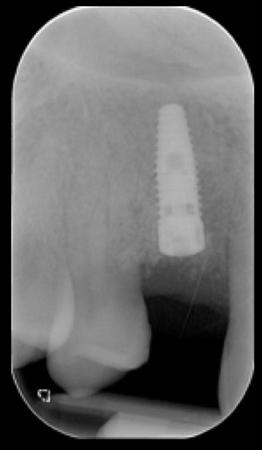
The lateral incisor exhibited a broader periodontal ligament (PDL), mobility class II and periodontal attachment loss up to 9 mm. The surgical solution was the removal of the remnants of the failed bone graft, guided bone regeneration (GBR), implant insertion, and mucogingival plastic surgery to boost the biotype. A lithium disilicate (IPS e.max®) single crown restoration was used in this case.
Evaluation & Diagnosis


Treatment Planning

Progress & Completion





Follow-Up & Outcome





Questions
Ask a questionWhat were the occlusal contacts on tooth 13 after the crown installation?
Hello dr. Great job, here. I’d like to know more about the occlusion on that tooth, #13. After you installed the final crown and after 4 years follow-up. Thank you.
Hello dr. Great job, here. I’d like to know more about the occlusion on that tooth, #13. After you installed the final crown and after 4 years follow-up. Thank you.

Dear Petronela,
thanks for asking....your question is really important!
A mutually protected group function was achieved in order to protect the right maxillary lateral incisor from occlusal trauma.
My Best Regards,
Giorgio Tabanella
You mentioned you did mucogingival plastic surgery to boost the gingival biotype. What did you do and when?
You mentioned you did mucogingival plastic surgery to boost the gingival biotype. What did you do and when? I am also curious how you resolved the 9 mm of attachment loss you had on the mesial of the lateral incisor. Some would have removed #7, included that site with the GBR and constructed a two unit bridge with #7 being a cantilever. Did you consider that in your treatment plan?
You mentioned you did mucogingival plastic surgery to boost the gingival biotype. What did you do and when? I am also curious how you resolved the 9 mm of attachment loss you had on the mesial of the lateral incisor. Some would have removed #7, included that site with the GBR and constructed a two unit bridge with #7 being a cantilever. Did you consider that in your treatment plan?
Dear Stephen,
the mucogingival plastic surgery to boost the peri-implant mucosa was performed at the time of uncovery.
The technique I utilized is called "The Buccal Pedicle Flap". It will be published on the International Journal of Esthetic Dentistry Volume 14 Number 1 Spring 2019.
The technique is minimally invasive, it does not require any CT graft, it can be applied for anterior and posterior as well as single or multiple implant sites. The technique can increase the mucosa thickness as well as the band of keratinized tissue.
Please don't hesitate to let me know if you need further info.
Regards,
Giorgio Tabanella
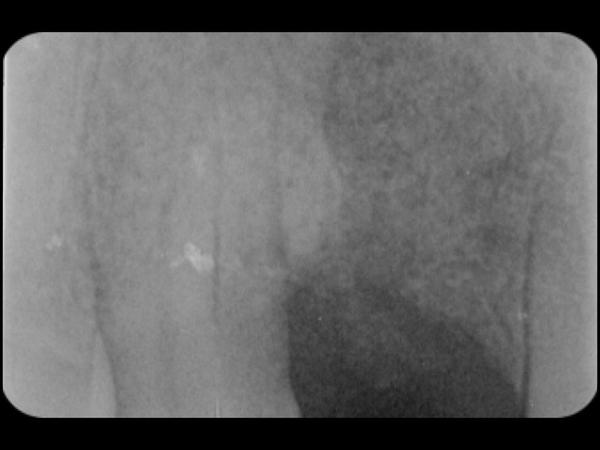
Sir,The results of this case are mind blowing..I would like to see a radiograph of the treated site sir... coz most of the times an Implant is not indicated at a site adjacent to a Periodontaly compromised tooth...
How did you resolve the 9 mm of attachment loss on the mesial of #7? Did you consider removing it and doing a cantilever bridge?
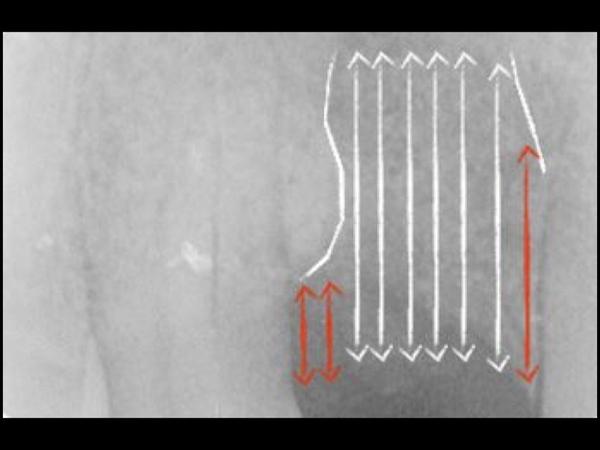
Tooth #7 had a poor/guarded prognosis due to attachment loss so an extraction was planned at the beginning as well as implant placement in area #7.
However by extending the recipient site not only at the level of the edentulous area but also palatal to #7 it was possible to obtain a repair: no periodontal pockets were reported after GBR. After a follow up of almost 6 years from the delivery of the final restoration the periodontium on #7 is still stable.
My Best Regards,
Giorgio Tabanella
Why did you use uncomon form for this crown? Why did you change the top of this tooth?
I would like to know what causes a "creeping attachment" and will the gingiva eventually remodel?
Test

What bone graft material did you use and what did you use to hold the graft?
In reply to What bone graft material did you use and what did you use to hold the graft? by Leslie Tu
What is the muco-gingival technique used in this case
In reply to What bone graft material did you use and what did you use to hold the graft? by Leslie Tu
Dear Leslie,
thank you very much for your question!
I used 50% autologous bone and 50% xenograft (demineralized bovine bone). The autologous bone was harvested from neighbouring areas by using a micro-harvesting tool.
Don't hesitate to contact me if you have any further question.
Regards,
Giorgio Tabanella