Maxillary central incisor: Immediate implant placement and periodontal plastic surgery
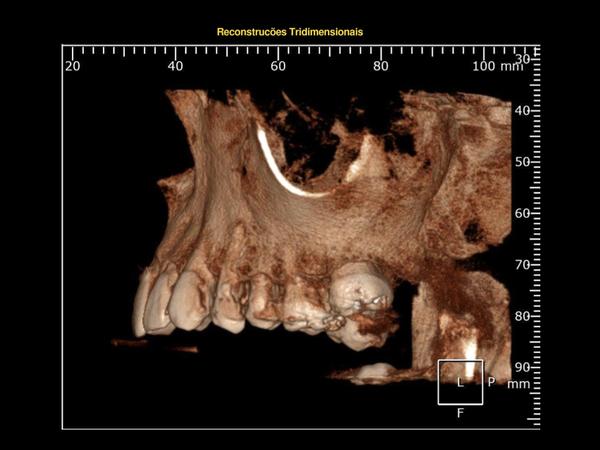
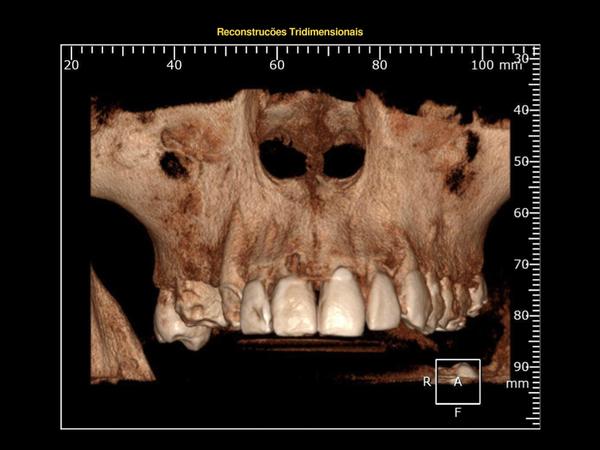
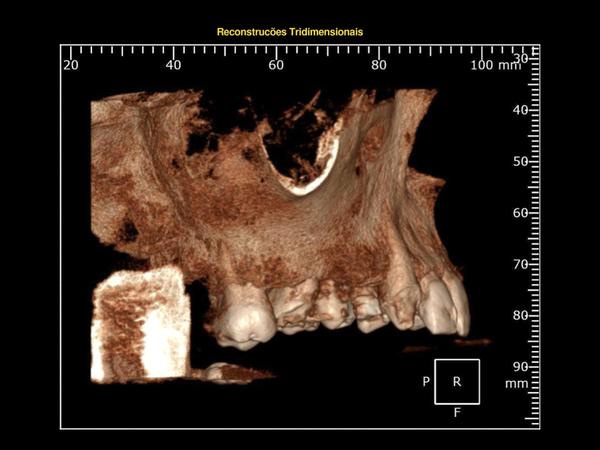
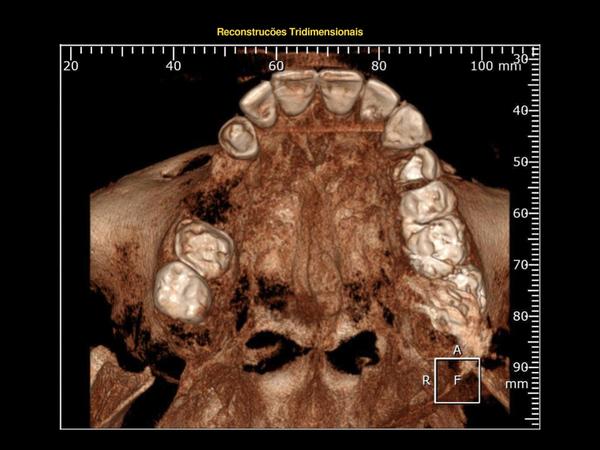
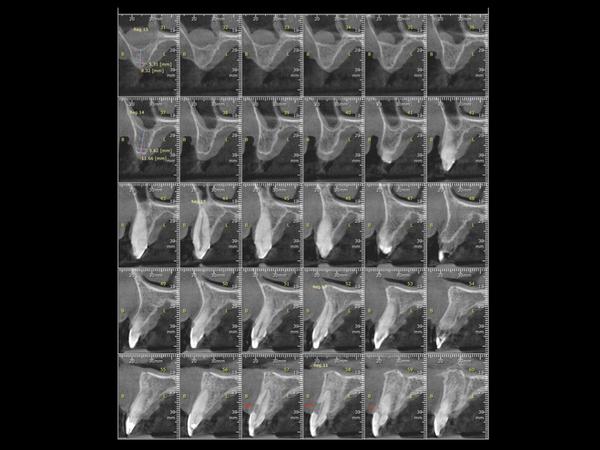
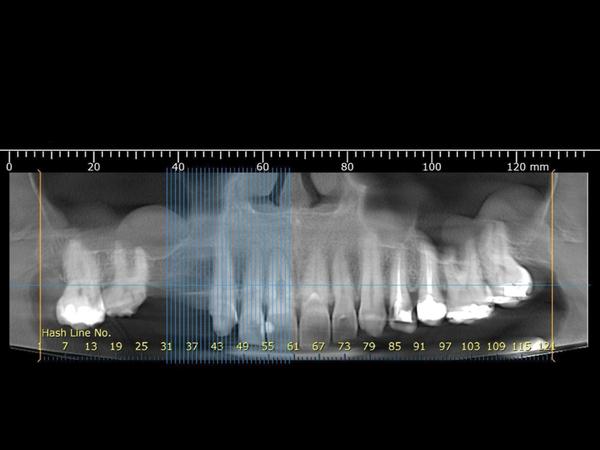
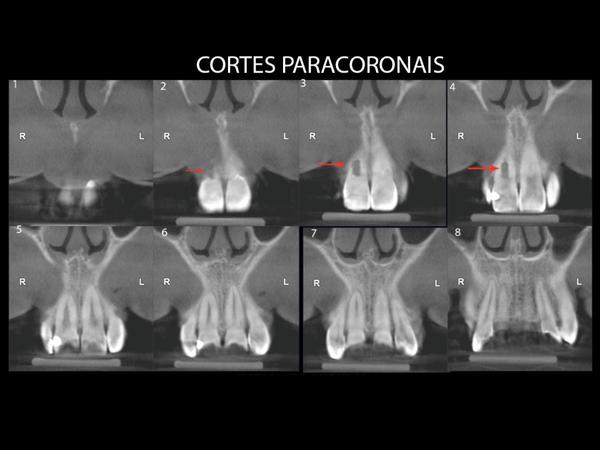
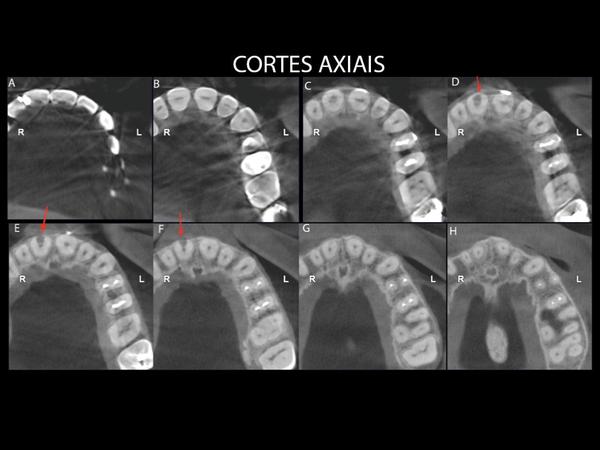
A 37-year-old female patient presented with a 5.0 mm periodontal pocket on the facial surface of the right central incisor with moderate periodontal inflammation. After a CBCT scan was performed, external root resorption was discovered on the facial surface which required tooth extraction. It was observed during the clinical examination that 3.0 mm of gingival recession was present on the facial aspect of the left central incisor.
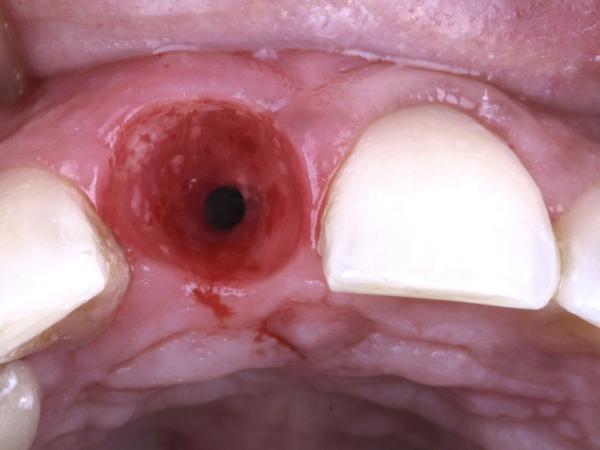
The objective of the treatment was to replace #11 FDI (#8 US) using immediate implant placement and to perform root coverage of the #21 FDI (#9 US) using a connective tissue graft.
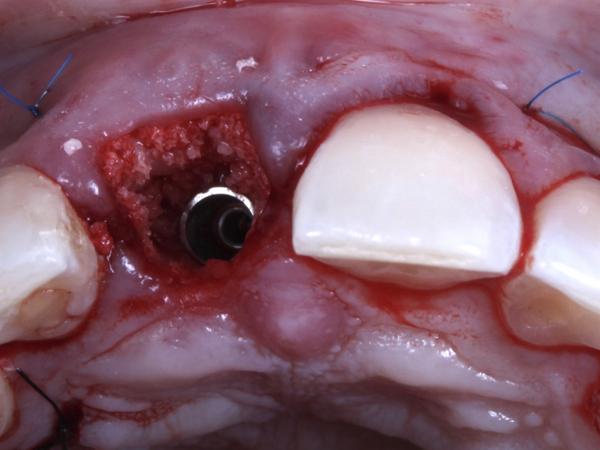
A NobelActive regular platform (RP) 3.5/13 implant was placed, with a temporary abutment. Geistlich Bio-Oss was placed in the gap between the implant and bone. The definitive restoration was fabricated using a Universal Base and 1.5 mm abutment height, a zirconia individualized abutment, and a lithium disilicate (IPS e.max) ceramic crown.
Evaluation & Diagnosis



Treatment Planning
Progress & Completion







Follow-Up & Outcome





Questions
Ask a question
extraction can be avoided
extraction cannot be justified.
i feel tooth can be saved.
lot of options available for saving teeth
extraction cannot be justified.
i feel tooth can be saved.
lot of options available for saving teeth
Given the relatively large size of root resorption, how would you predictably save the tooth without the of risk of delayed intervention and then jeopardising the relatively intact buccal plate of bone with possible further bone resorption?
Agree with Ramzi, the extension of the resorption and the begging of buccal bone loss was the main issues that de Endodontist indicated the extraction.

Was an Endo opinion taken before extracting the tooth?? To avoid medico legal scenario.....
The shape of the crown during cementation and at the 1-year recall appear to be different.
Fantastic results. Absolutely loved it. One question I had was - the shape of the crown after cementation and the shape at the 1-year recall appear to be different; the crown is more squarish in the cementation photo. Were any changes made? Also, in retrospect, is there anything you would do differently if you had to do the same case all over again? Thanks in advance.
Fantastic results. Absolutely loved it. One question I had was - the shape of the crown after cementation and the shape at the 1-year recall appear to be different; the crown is more squarish in the cementation photo. Were any changes made? Also, in retrospect, is there anything you would do differently if you had to do the same case all over again? Thanks in advance.
Just the picture, there were no changes in the crown. Today I would go for sure with Guided Surgery and a milled provisional.


Justification of the the Extraction
Comments:
1. The Implant Platform diameter discrepancy corresponding to the 11 root diameter at ECJ!
2. Lack of LCPPA radiograph before and after and follow-up!
3, Simultaneous correction of the recession of the adjacent tooth 21!
4. Extreme vicinity Prov. rest. margin to the Implant-abutment interface or Bone margin violating the Biological width!
5. Lack of GBR technique in the presence of Straumann bone Ceramic (membrane?)!
6. ..............
Comments:
1. The Implant Platform diameter discrepancy corresponding to the 11 root diameter at ECJ!
2. Lack of LCPPA radiograph before and after and follow-up!
3, Simultaneous correction of the recession of the adjacent tooth 21!
4. Extreme vicinity Prov. rest. margin to the Implant-abutment interface or Bone margin violating the Biological width!
5. Lack of GBR technique in the presence of Straumann bone Ceramic (membrane?)!
6. ..............
In reply to Justification of the the Extraction by Nico kamosi
Hello Nic, regarding to your topics.
Extraction: large resorption with some crestal bone loss and no predictability to any treatment to stop that. The endodontist that indicated the extraction.
1. As we place immediate implants in the aesthetic zone especially, we should leave at least a minimum of 2 mm of buccal gap, that was the motive to install the NP Nobel Active.
2. please explain me LCPPA. WE have a short follow up until now, but I will send here the latest as soon as I have it.
4.The biological width was intact, as the implant was 4mm above buccal mucosa margin. and you can see in X-ray that there was only bone remodelling at the follow up and no bone loss.
5. In our practice, when the buccal plate of the extraction socket is from 3 to 5 mm from de gingival margin after tooth extraction, we just fill the Gap after implant insertion. No need of membrane in this case.
I hope was able to help